


Seroquel IV: Bipolar Depression
The quelling of the hot blood is good, but what about the icy depths of depression?

“Being on Seroquel was the worst. I used the metaphor of being turned to stone. I slept for 14 hours a day but was still psychotic. Eventually, I learned to shut up about my delusions, so they could discharge me.”
— A Patient Reflecting on Experience of treatment with 700mg of Seroquel in an inpatient psychiatric setting.
***
This is the fourth part of our series on the drug Seroquel. Prior articles include Part One, about the medicine’s use in schizophrenia, Part Two, regarding its (attempted) use in borderline personality disorder, and Part Three, a brief aside about the name of the drug, are linked here for your convenience and pleasure.
Given the comprehensiveness of this piece, I decided to release it on Monday morning, after spending the weekend writing it. It's like I took a weekend off, without actually taking the weekend off. That's how much I love my readers.
In the of bipolar disorder, we have two separate mood states. One of them is depression, and the other is mania. After the initial approval for schizophrenia, Seroquel was put through its paces in bipolar disorder mania, followed by depression.
TL:DR; it's an effective treatment for both.1
Sidebar: Dopamine Receptor Blockade and Side Effects
As a dopamine blocking medication, at the dopamine D2 receptor, Seroquel is most similar to clozapine, the first of the second generation and the psychotics in its receptor binding profile.
It has what we call “loose binding2”—it's hang out for a little time on the D2 receptor, dissociates, and then pops back on. There is an equilibrium of receptor-bound and unbound quetiapine in the synapse, and this level never gets above about 60%. That number is evaluated in living humans with the use of PET scans, as I described in one of my 6️⃣ previous article about Abilify.
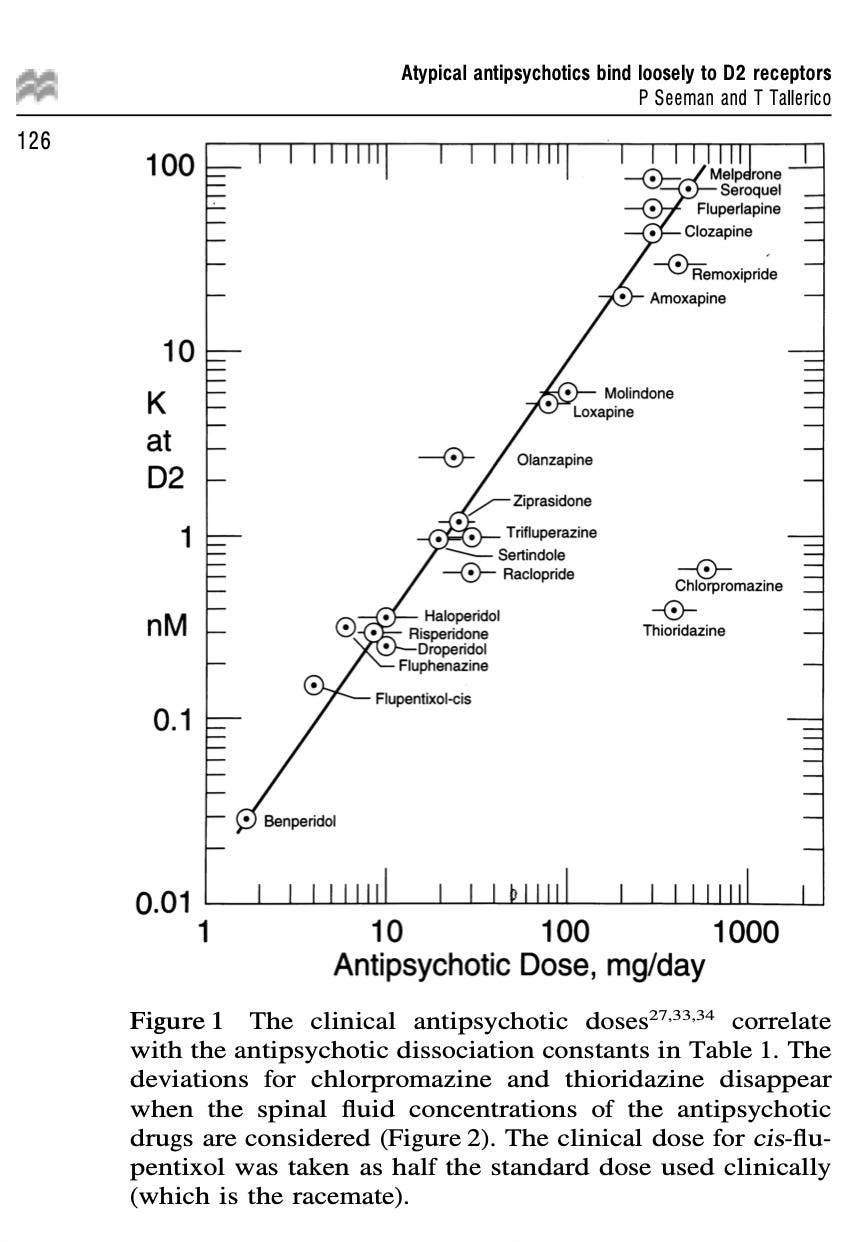
If it wasn't for the initial efficacy of clozapine, no one would believe this drug worked, because the orthodoxy was that you needed a greater than 60% receptor occupancy, to achieve anti-psychotic efficacy. Above 70%, and you start running into extrapyramidal symptoms (EPS for short), Parkinsonism, other movement disorders, and various nasty side effects.3
Which nasty side effects you ask? Rigidity and dystonia—that's an involuntary contraction of muscles on both sides of a joint so that the part of the body doesn't move. These are all much more common side effects with drugs other than Seroquel.4
Seroquel Adverse Effects…At Scale
One of the sticky wickets about drug development? It might seem obvious after I write it, but it is worth spending a moment with. Before a drug’s FDA approval, we have no information about what it will do when given outside of clinical trials. Clinical trials answer some questions extremely well, and others….not so well.
As someone who runs clinical trials, I am interested in adverse events. Each one, big or small, is a big enough deal to take notes. These notes on “Treatment Emergent Adverse Events” (TEAEs) and “Severe Adverse Events” (SAEs) are dutifully logged. In a recent trial, I had a few patients in a row who had no adverse effects at all! I got a call asking if I forgot to log them. We “trialists” are really into tracking “AEs.”
One thing sticks out to me in reviewing the submitted data to the FDA—which again, I'll emphasize is publicly available to us all.
I'm not quite sure at this point why medical school isn't mostly learning how to read through these filings so we know what's bullsh*t and what's not for a year? Way, way more time in medical training should be spent digging through submissions to the FDA, if it were up to me!
Another thing that sticks out, about Seroquel, is how good those early studies were in picking up adverse effects that were going to be problematic at scale.
Let me walk us through some of those adverse effects as submitted to the FDA, and then we'll get to the efficacy data after it went to market. After approval? It is a huge uncontrolled experiment. It’s in the people who would have been screened out and in whom adverse effects are much much less carefully tracked.
Effectiveness—does this improve my life?!—becomes the important question along with safety at scale.
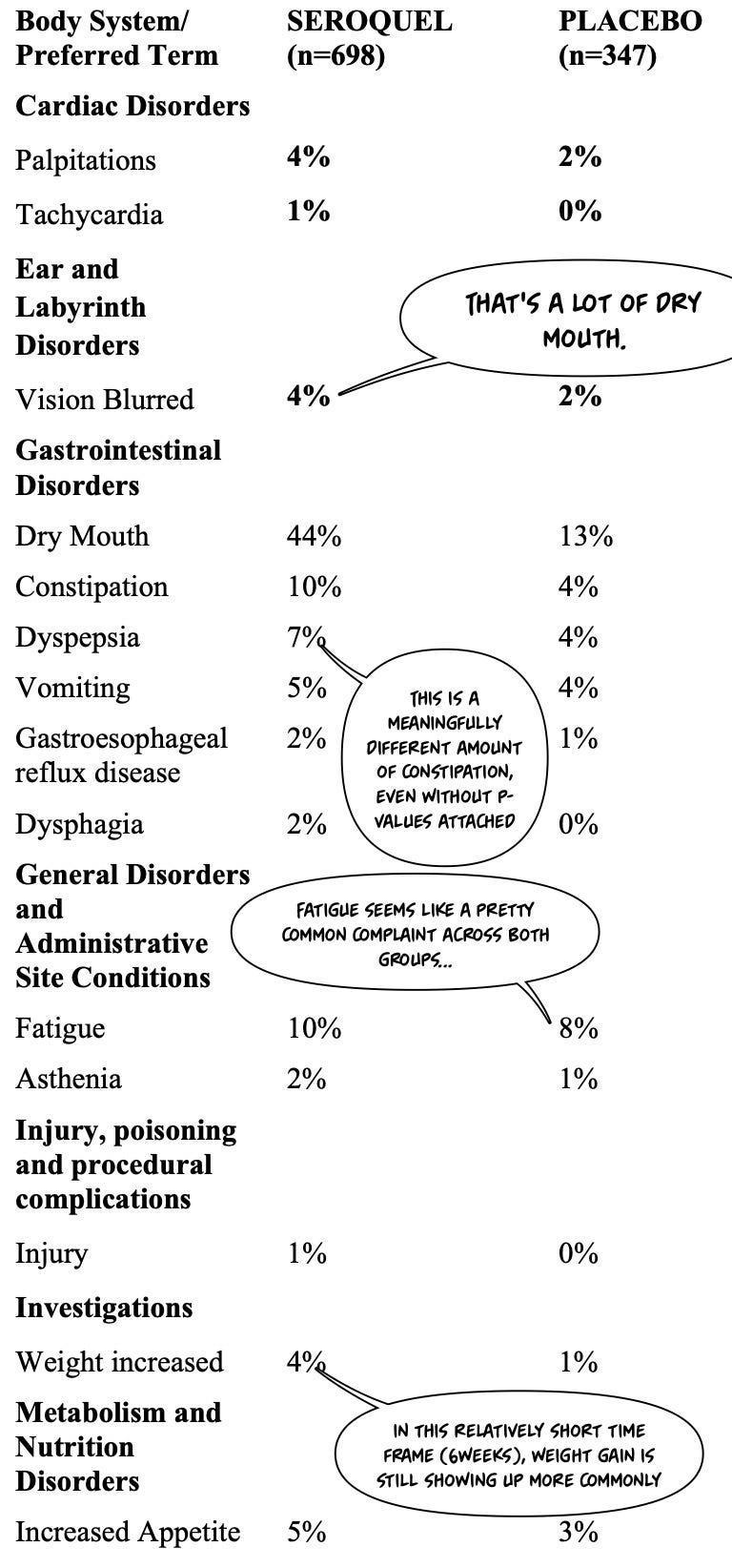
Let's start with the submitted adverse effects:
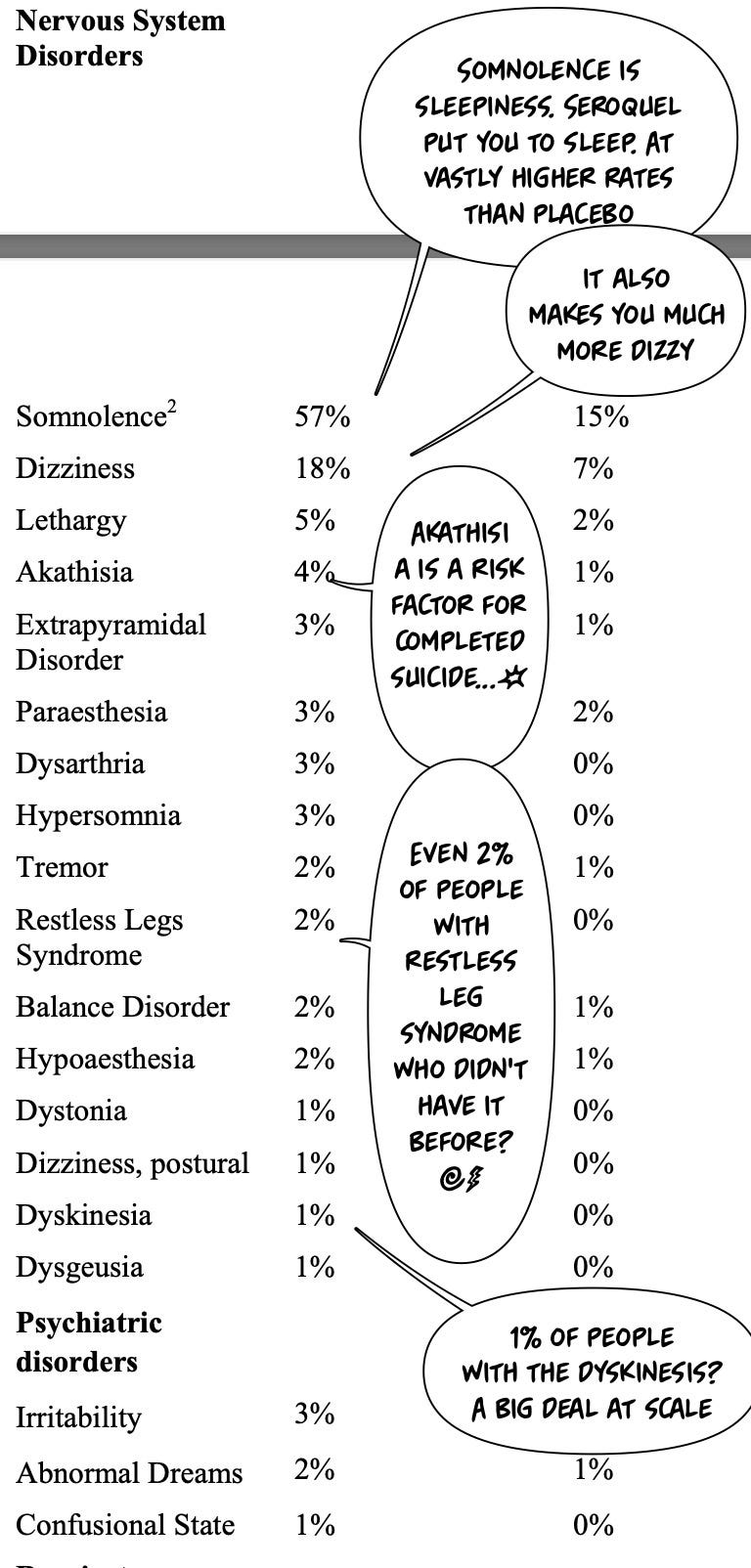
Let us continue with the impact on the nervous system. Seroquel is on the left, placebo is on the right.
Comparing those adverse effects in the nervous system specifically to risperidone (link to previous awesome article and podcast!) another atypical antipsychotic, we can see how different Seroquel is…
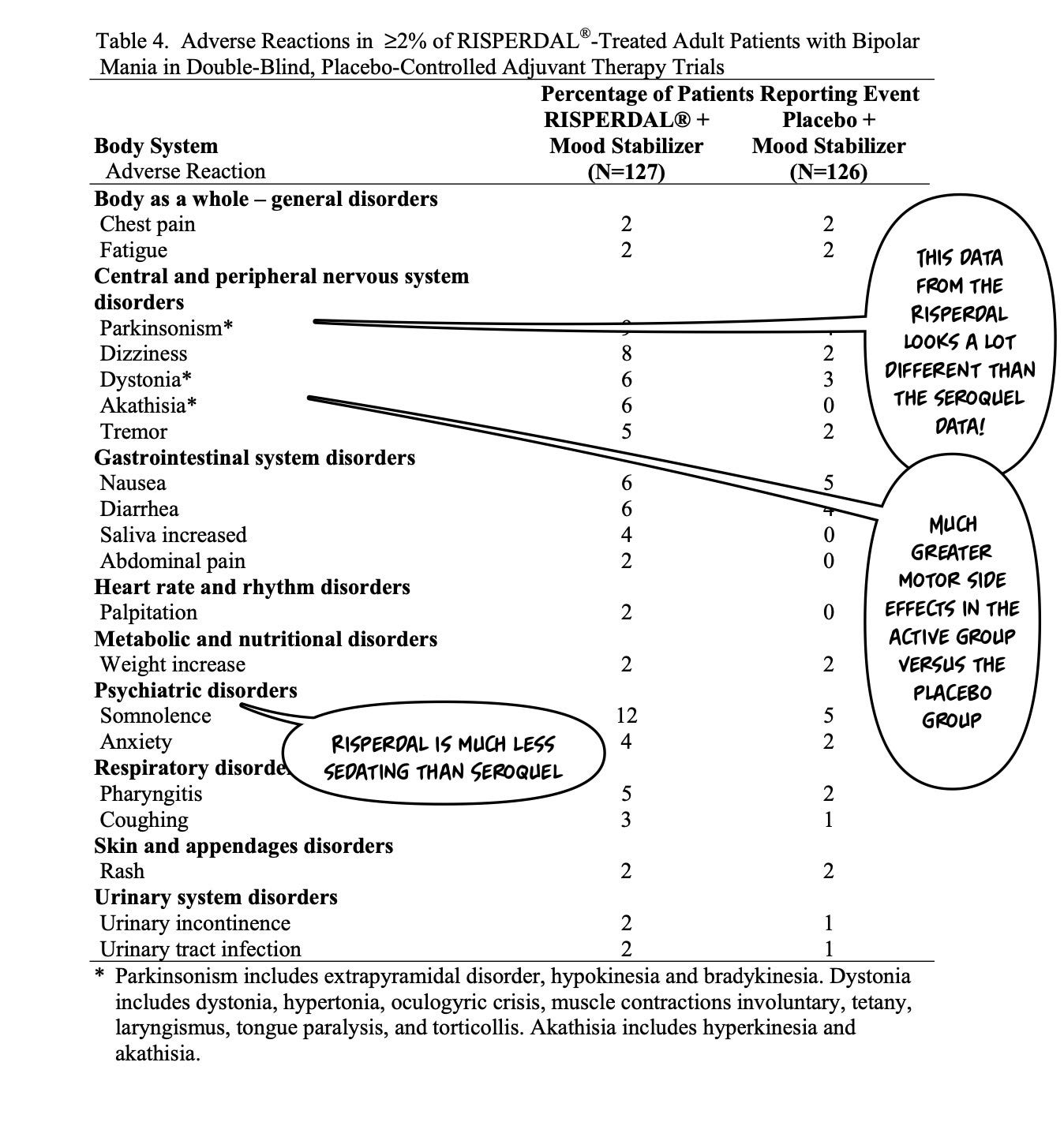
Especially when you compare those very specific rates of adverse effects in Seroquel versus placebo around its impact on the motor system, where it is not as bad as placebo!
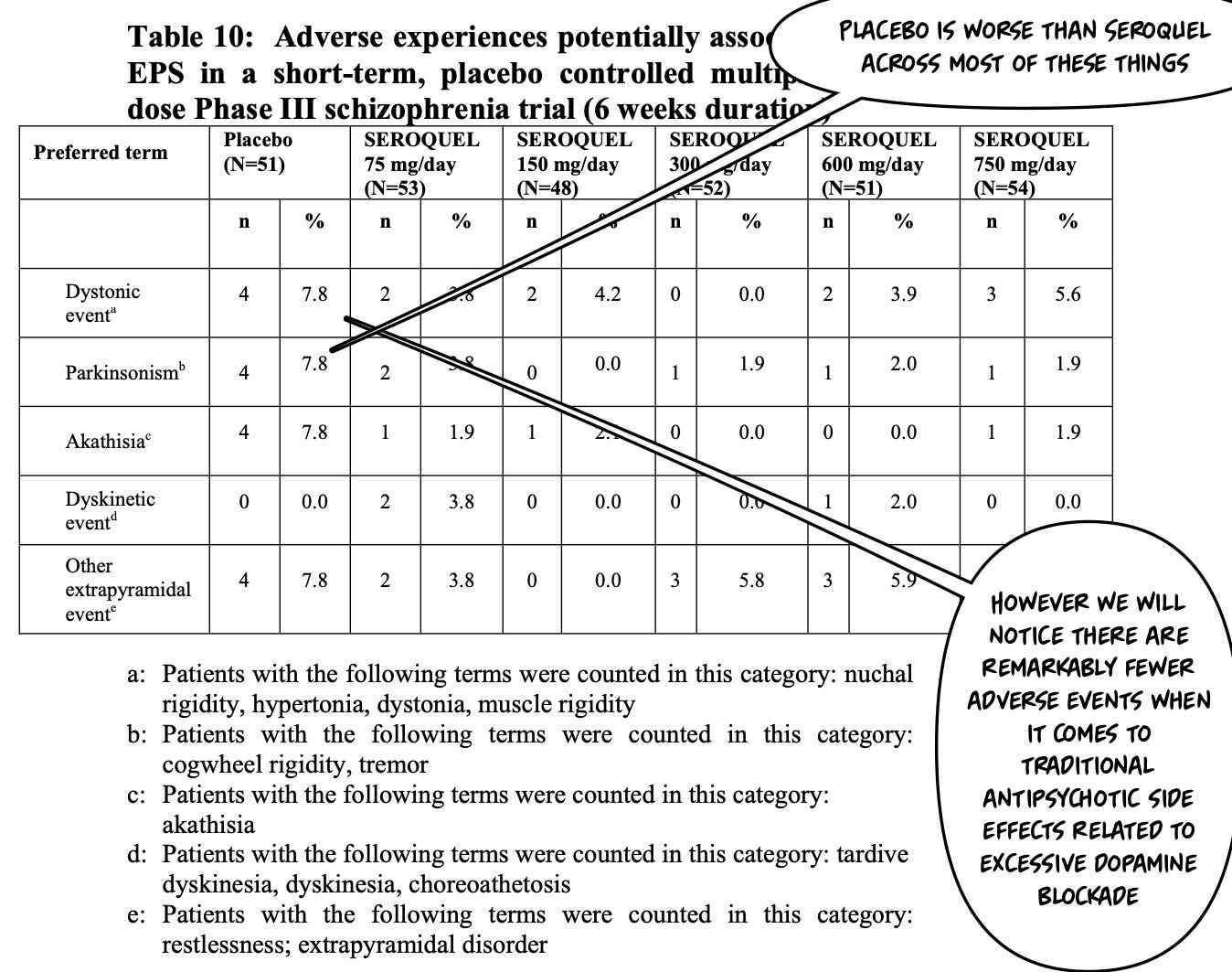
Even though this drug is working as an antipsychotic, and binding dopamine receptors, we're not seeing the same adverse effects as most antipsychotics. It's much more metabolic dysfunction and sedation compared to almost everything that came before it—with the possible exception of clozapine!
The downside? It it's not as effective as clozapine in schizophrenia, but may do something special in bipolar disorder…
Before we get to all the good things it does, let's finish with the risks and warnings from the FDA, and think about whether physicians are routinely warning their patients appropriately?