


An Open Letter to UnitedHealth Group after Declining My Employment Application: Redux
As Inspired by Rage Against the Machine Live @ Madison Square Garden.

Today is a day where we all get to reflect. It's actually true about every day. Recently, the CEO of UnitedHealthcare, which is only a subsidiary of United Health Group, the actual overarching company, was murdered in the streets of New York. The public has been deliriously and overwhelmingly thrilled to celebrate the death of an employee of a major public company. I've been on the “UnitedHealth Group has deplorable business practices” train for a long time, so it's with only grim satisfaction that I notice that everybody else hates big health insurance— but doesn't understand how it works.
I have a lot of articles about that! I've written over the past 2 1/2 years on the topic. Today's recycled article is one such piece of satirical writing, but if you want a good overview of everything wrong with insurance, a couple of prior classes will get you there. The most important concept is the Medical Loss Ratio and how it's shaped health insurance business plans. I write about that in this article, where I compare it to the Passion of the Christ. I explained the Pharmacy Benefit Managers at the heart of the insurance scam, comparing them to the Mafia. I've explained how the CEOs (yes, they are plural) and other executive leadership of the United Health Group may have the crime of insider trading in this post here. I have reviewed the dubious hiring/firing practices of UHC with this original reporting. I’ve explored the scope of Optum’s Change Healthcare subdivision. I’ve explained absurdist schemes to manipulate the stock market as a joke, as an excuse to explore why everyone should bail on UHC for their health plan. I’ve even pilloried Sauron for insider trading as a way to poke fun at UHC. Those pieces, and hundreds of others, are well worth reading at this point. Today, I will share one of my all-time classics and one of the most popular pieces I've ever written: my open letter to UnitedHealth Group making fun of their casual relationship to employment law. I will again emphasize that cheering for the murder of somebody in the street is not what we should be doing. It's not only ennobling the least noble instincts humans have—while glossing over the fact that the person killed will now never be a witness for the government in prosecution against others at his company for insider trading—but it encourages others to commit murder. As a Psychiatrist, I'm here to tell you that when you pay attention to behavior, you get more of it. It doesn't matter what kind of behavior it is, but when you pay attention to anything, that action is rewarding. There are plenty of angry people armed with guns in America, and they're watching somebody get lionized in the press, and on social media, all day long, being called a hero. Maybe we can imagine that's not going to spread? But I very much think it will. When we cheer for murder, we get more murder. More murder is not good. I am surprised that this is a controversial stance, but 2024 has been weird. Thank you for reading this over a long introduction, and now some satire for all of us to kick back and enjoy on a Saturday.
It will come as a surprise—to absolutely no one—that this column’s narrator, the eponymously named “O. Scott Muir,” has a real penchant for gonzo journalism. If “considering the lobster”1 was a profession, I would’ve probably been licensed by now.

Somehow, I got a medical license2 instead, so I’m stuck poking around the healthcare establishment for unorthodox perspectives3 and sassy think-pieces.45
In prior writing, I spent a significant amount of effort on getting just the right degree of snark infused. Generally, this snark pertains to “less than ethical” practices by Big Healthcare. But today, I can say—in all honesty—one of the giants made an unimpeachable decision. At some undisclosed point in the past, the following email hit my inbox (this is a WIN, though, as we will see, perhaps not in the way it first appears):
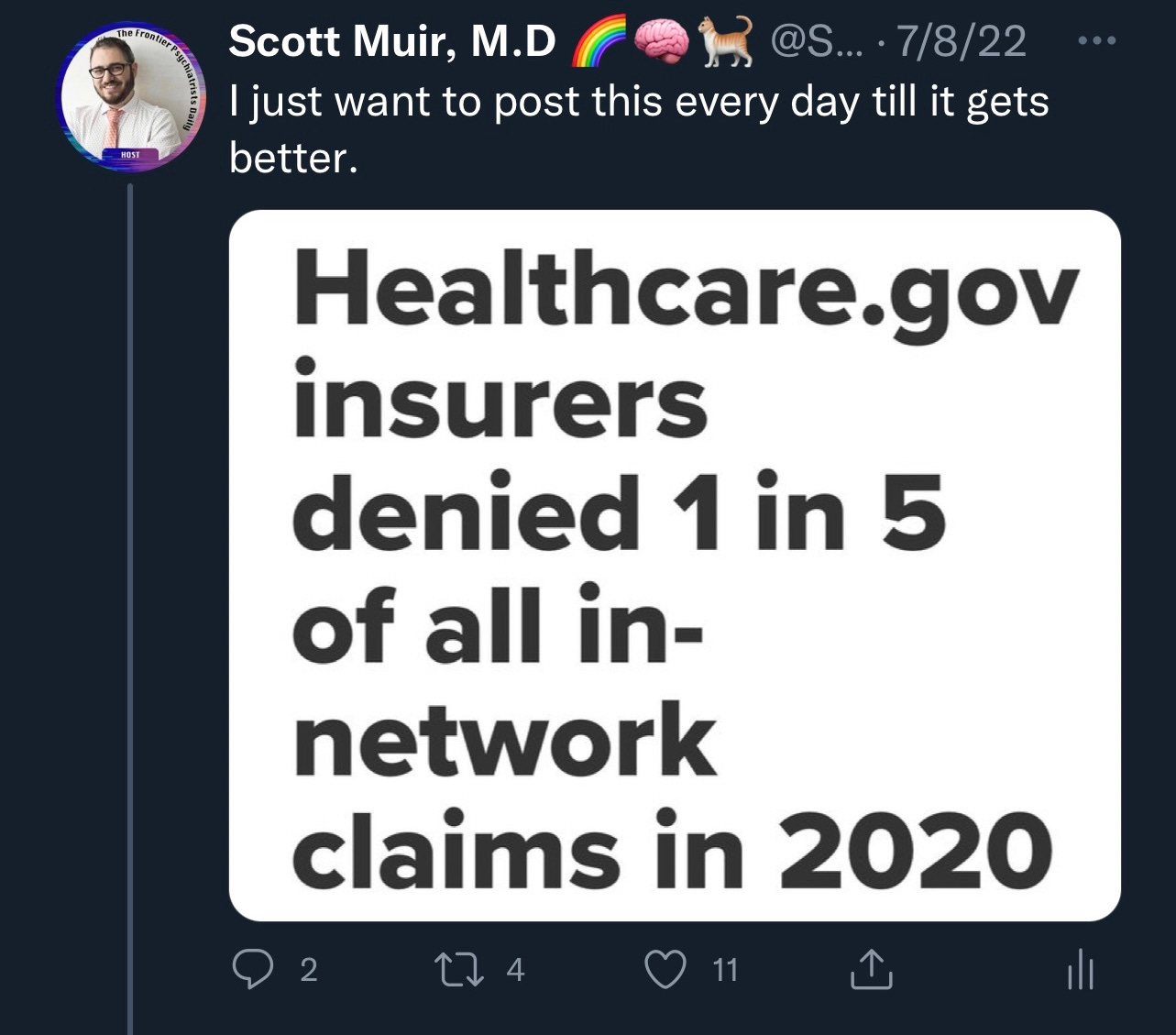
UnitedHealth Group made the decision to decline my job application for an open Behavioral Medical Director role. I may have seen it on LinkedIn. I may have applied on a bit of a whim. This “hard pass on me” is a great-ish call on the part of talent acquisition. As anyone who’s read this column or my Twitter can tell, I’m not a huge fan of their business model:
I’m not saying I was unprofessional in my intent to interview. However, my pre-test probability for “how likely the interview process was to change my mind” was not high. And, frankly, I don’t know how ardently I would have been able embody my new (and presumably fiduciary) role to UHC Shareholders.6
For example, I might have been tempted to point out problems such as: “There’s no such thing as a Behavioral Medical Director.” Medical Directors are doctors. The term, in the field of medicine, is psychiatry. This is, for the uninitiated, a medical specialty dealing with behavior. We understand this as the output of brain function—it’s our organ system of interest. It’s like advertising for a Urine Medical Director7 for a Nephrology service line.
The most unsettling part of this now-distal-but-still-haunting rejection, which I am trying to deal with through the mature defense mechanism of sublimation, is the fact that, not only is it less likely that I will be doing my life‘s best work, but it is, in fact, guaranteed. United Talent Acquisition has trademarked that very phrase.
🚨 The only place I can legally pursue your life‘s best work (SM) is at UnitedHealth Group. 🚨
Moreover, because this slogan is intellectual property owned by UnitedHealth Group, it’s the only place anyone can do their life’s best work.
Take a moment. Clear your mind. Breathe in, breathe out.
Feel the breath exit your body.
And now, slowly, and with renewed focus and clarity, return to the abject horror that is the legally sanctioned state of the world in which meaning is the property of UHC.
The Context, Which Frames Nicely Why This Rejection Letter Is, Despite the Jocular Tone of This Writing, Felt Sincerely
I’ve spent almost 60,000 hours of my life as a practicing physician. The work I do is so defining, both in terms of who I am and what I will be, that the need to create a better world is almost all-consuming. I’ve sacrificed more time with friends and family than the hours you have doom-scrolled on Twitter and Facebook combined. I’ve built companies and sold them8. I’ve mourned the death of humans, including some in my care, who died by suicide.9 I’ve shared tears of joy with patients and families as they succeeded. I’ve seen former patients become colleagues! I’ve stood on stage with friends, colleagues, and patients as we rang the bell at NASDAQ for public companies I’ve worked with. I’ve experienced remarkable art borne of data I’ve collected10. I’ve been accused, along with my wife, of rape and murder, in a mendacious lawsuit11—in which deeply unscrupulous lawyers12 exploited the grief of a parent who lost a child to suicide after literally thousands of attempts that we, as a patient, family, and physicians, went through together—only to have it dismissed with prejudice. I subsequently had the case appealed to the higher court! We had to file for it to be returned to the active docket, so that it could be heard. This is all because the plaintiff was too busy harassing me on Twitter to move forward with her own case.13 I’ve been stalked by an individual using email addresses both profane and implausible.14 That stalker has threatened to murder me on my birthday.15 I have known the joy of inspiring young medical students—themselves feeling hopeless after a psychiatric diagnosis—by the public disclosure of my own life with bipolar disorder.16 I’ve published remarkable17 findings1819, and seen them replicated20 in what I see as a sea change in the field of psychiatry. I've seen these findings lead to an FDA Breakthrough Treatment21. I’ve had ups22 and downs23, the scale of which beggar belief.
I will have to find a way to explain all that to my children as they become old enough to search the internet for their parents and find an entire, somewhat absurd blog24 dedicated to ruining my life. I’ve had investors pull out of millions worth of investment because they were worried of what other people would think of said blog. I’ve watched my wife’s company become one of the most successful, acclaimed start ups of the day, despite all that. As the kids would say, it’s been a lot. And now, I must confront the following and somehow make sense of it.
Which work is off the table? You know, the best work. This is it. The only place. Kiss your academic dreams goodbye. Forget entrepreneurship. Semi-academic child psychiatry non-profit fiefdoms? No! It’s at UnitedHealth Group that that’s going to happen or not. At all. It’s work at United or… (quoting from the inscription above the gates of Hell itself, from The Inferno, because who is literate but also damned to eternal toil? This author, apparently):
“Through me you enter the city of woe:
Through me you enter eternal pain:
Through me, you join the souls, lost.
Justice, it was, that moved my maker:
To raise me, with divine power,
Supreme wisdom, and primeval love.
Before me, there was nothing save the
Eternal, and eternal I remain.
Abandon all hope, ye who enter here."25
And This…This Is the Stuff of Existential Crisis, or 90839, as CPT Coding Would Have It
What was surprising to me? This was clutch IP26 I was unaware of this, prior to submitting my application. It’s not that UnitedHealth Group as the owner of meaning in the lives of healthcare innovators is widely broadcasted. In fact, the first time I became aware of this IP was upon my application having been received.
I was invited to submit voluntary disclosure27 of my disability status28, which I did. As a federal contractor, this is mandatory. After which, from an HR perspective, I think it’s a little bit strange that the next communication was to tell me that this isn’t where I would be welcome.29
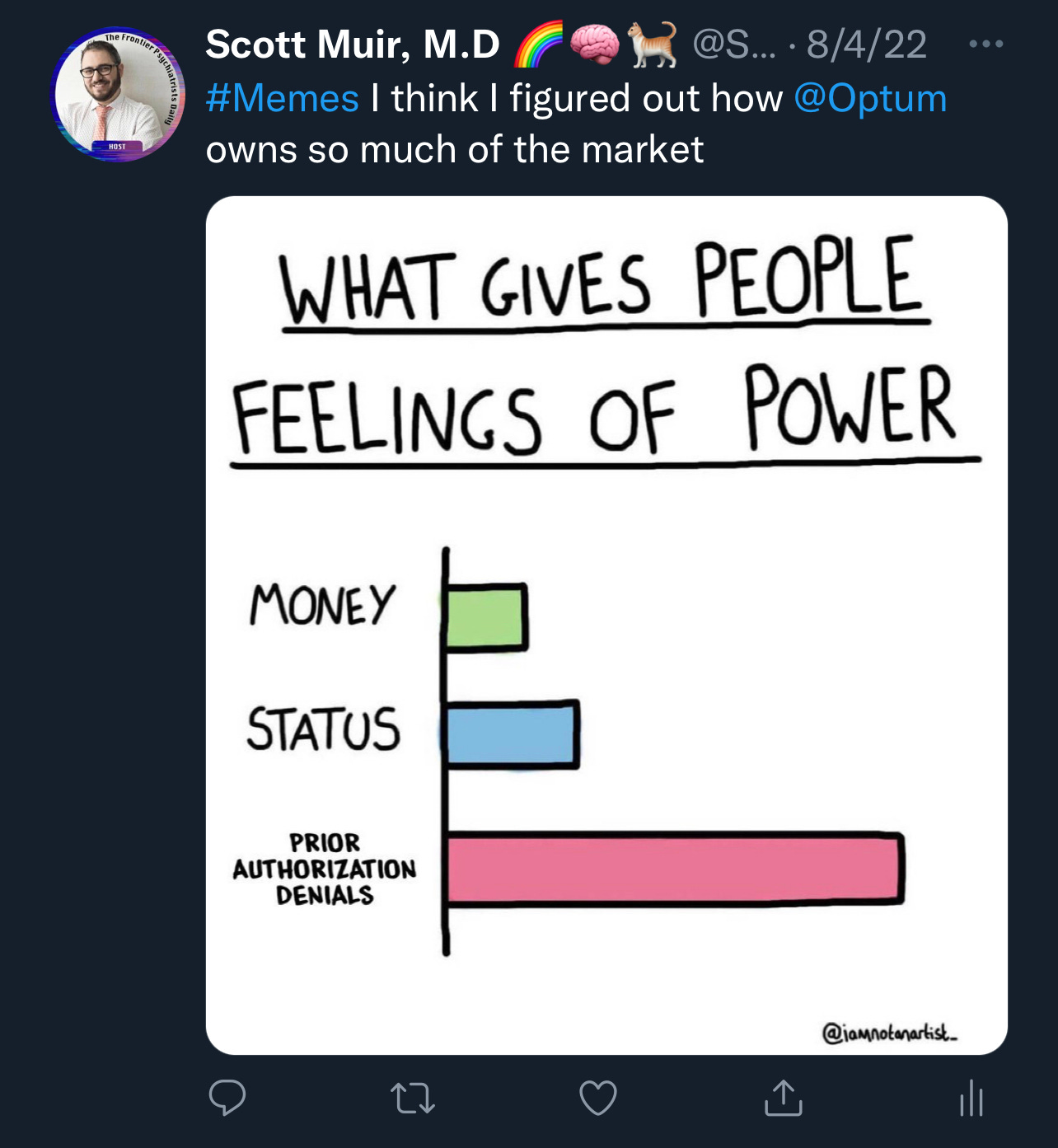
As much as I think that even a casual inspection of my comments on Twitter and social media, regularly 💩posting Optum,30 is a pretty ok, maybe even excellent, basis for considering other candidates, it does seem like now would be a great time to review what I had hoped—now utterly in vain— to be my Life‘s Best Work (SM). Work, tragically, I now must leave behind me.31
At times like this, I find succor in the unexpected. Comfort is forthcoming; wait for it, from none other than UnitedHealth Group! Coping, made manifest in a relentlessly corporate blog post. And—this is literally and inexplicably true—United provides perplexing, invalidating, vexatious advice on the mechanisms by which humans might “laugh” or enjoy “humor”:
Sure, life can be stressful at times, but32 the simple act of laughing at a stressful situation can make it easier to cope. Laugh at yourself—we all do some silly stuff and having a good sense of humor about it is a great approach. Find something to laugh about every day—and if anyone asks what’s so funny, have a few jokes ready to help spread the joy.
Thanks, United! UnitedHealth Group advises—when the going gets tough—to laugh at ourselves. The good news is, I have moved on and committed myself to pursuing my life’s second-best work.33
Abandoning My Life’s Best Work Gem #1: More Robust Prior Auths!
Among the least quotidian tasks I would’ve accomplished—had I been allowed to pursue my Life‘s Best Work (SM)—would have been the refinement of prior authorization workflows. As a public service, my vision for the future prior authorization follows, and anyone at UnitedHealth Group is welcome to it. It might not be my Life’s Best Work (SM), but it could be yours:
Every time UHC requires a diagnosis for a treatment or procedure to be approved, it is guaranteed that every submission will have that diagnosis. I’m not sure which percentage of these are lies, but I promise you it’s more than 0%. I think this is an area of growth for Optum Insights, the subdivision of the United-Healthcare-multi-headed-hydra that is responsible for data analytics.
My humble proposal is generating natural language processing software that can access prior medical records to restrict clinicians from making up diagnoses that fit with prior authorization requirements. This way, many many more treatments will not meet criteria for approval, without the manual labor of having to do peer-to-peer reviews to figure out if doctors are BS-ing you just to get their treatment approved. This happens all the time. You’re welcome.
Abandoning My Life’s Best Work Gem #2: Our New “Approve a Claim, Deny a Claim” Program!
It stands to reason, given the number of times Owen Muir, M.D.34 has punked prior authorization reviewers by questioning their experiences in my particular field of sub-specialty—and then used that as leverage to advance to the next level of appeal—that a system in which every in-network physician who submits claims also functions as a conscripted claims reviewer would be baller. It both crowd-sources the process and serves as a bulwark against successful arguments! Similar to buy one, get one free offers, as long as we make the criteria for authorization of claims unofficially the denial of more claims, you create a conscripted-shadow-cap-and-trade system for care! It gives every interventional sub-specialist the incentive to use their expertise to deny authorization requests from colleagues. If we keep tinkering with numbers, everyone will start gaming things out in ever more economically productive ways… for UnitedHealth Group of course! As much as this is meant to be comical, the amount of time they force us to waste fighting their denials right now isn’t paid, and it is work we’re doing for their bottom line as it is. This is not actually more crazy.
Abandoning My Life’s Best Work, Gem #3: Rage in Favor of the Machine and Its Subsidiaries!
Ok, I may have snarked as much snark as I could possibly snark. UnitedHealth Group is a big company. Here is how insane their incentives are:
They can set up a system that intentionally dances with class action litigation around disability discrimination (see footnotes) in a wildly expensive jurisdiction for that kind of activity.
They can similarly suborn systematic retaliation (see footnotes) in hiring practices. Even this article is plausibly fuel for that fire as a piece of regulatory performance art.
They can even commit a level of ghoulish violence against all that is good and holy in design and typography with corporate email headers as follows, while having a straight goddamn face:

All of the above could be litigated, and even lose billions.

And those expenses, all of those expenses, would find their way to the UnitedHealth Group balance sheet in a way that increased the total cost of doing business for their health insurance business, and thus increased the amount of profits they were allowed to make using a fixed medical loss ratio calculation.
UnitedHealth Group = More Profits From More Expenses35
So I wasn’t being glib—this piece is to congratulate UnitedHealth Group: you have successfully avoided hiring a known provocateur,36 and done so in a way that demonstrates your rapacious hunger to be sued (seriously, see the footnotes), lose, and just make more money in the process!
I know Rage Against the Machine directs said rage against profiteering. This anti-machine sentiment has historically been directed at global arms sales. I hope the next time I get to see Zach de la Rocha in concert, I will get to hear the following:
Freedom? Yeah, right. More like:
Abandon all hope, ye who apply here.
—O. Scott Muir, M.D.
Consider the Lobster is a collection of essays and arguments by the inimitable David Foster Wallace. And yet here I am, in what is at best a pale, wraith-like imitation of him?
Name : MUIR OWEN SCOTT
Address : BROOKLYN, NY
Profession : MEDICINE
License No: 2xxxxx
Date of Licensure : 4/30/201x

What have those experts discovered? They found that laughter may increase circulation, boost mental function, decrease pain and stress, and release endorphins that help people feel happier. With all of those benefits, it’s plain to see that laughter is good medicine. (H/t UHC)
Full financial disclosure: I own just under 4 shares of UHC!

So, this whole thing is a deeply financially conflicted endeavor for us all, now isn’t it? Are those shares a hedge against the failure of this substack to take off? Or is this piece a hedge against my fear that, after being thoroughly underpaid for years by UHC as a physician—and owning so little United stock on account of it—that maybe, just maybe, I’ll get so many paid subscribers that I won’t have to keep hustling so hard? Sounds like… a call to action to me:
Next time, perhaps advertising for a Psychiatric Medical Director, and you might get a better sampling of applicants? Or maybe that’s what you’re hoping I would apply to? I was encouraged to continue applying to jobs at UnitedHealth Group, so maybe this was the problem…
The remarks I’m referencing are memorable, originally delivered in Washington Square Park. It closes with the bard thusly:
Our best known sensitive male teen fearing a life alone, Romeo, nailed the experience of abandonment in BPD while looking at the (actually sleeping) Juliet:
“For fear of that, I still will stay with thee,
And never from this palace of dim night
Depart again. Here, here will I remain
With worms that are thy chamber maids. Oh, here will I set up my everlasting rest,
And shake the yoke of inauspicious stars
From this world-wearied flesh.
Eyes, look your last.
Arms, take your last embrace. And, lips, O you
The doors of breath, seal with a righteous kiss
A dateless bargain to engrossing death.”
Suicide wasn’t being ignored in the Globe Theater in the 1700s. Let’s catch up to Shakespeare in recognizing tragedy. BPD kills people. Our silence makes us complicit, let’s cut that out.
The work is remarkable. It’s among the most remarkable pieces related to medical information I’ve ever experienced.
The whole lawsuit is breathtakingly sad. It is also, It is fair to warn you, written with a relaxed relationship to what would be traditionally understood as facts of a case.
The council for the plaintiff who filed the complaint, after having the case refused for manifest lack of merit by each medical malpractice attorney licensed to practice in the state of NY, had no prior experience in medical-legal matters. Furthermore, a wrongful death suit was filed after the statute of limitations expired and without a single physician witness testifying to the malpractice of the facts of the case. Thus, its subsequent dismissal.
However, the “with prejudice” nature of this dismissal emphasizes the exploitative and immoral behavior of this attorney, who is happy to take no small amount of money from grieving parents. Furthermore, it continues to highlight how vulnerable grieving parents are.
It cascades into the idea of how much lawsuits against doctors who care about suicidal individuals drive a gap in care. That gap is pernicious. Ironically, the most compelling reporting on this issue featured the very young woman who’s completed suicide as the source of the above complaint.
A dismissal with prejudice means that the ruling is the final judgment in the case. The dismissal prohibits the prosecutor from refiling the charges. In a dismissal without prejudice, the prosecutor can refile the charges (or file new charges based on the same circumstances) at some future time. However, the appeal was about if the lower court exceeded it’s authority in dismissing it with prejudice, and appeals court found that was the case. I have always wanted this matter litigated to shed the appropriate light on what happened, so when it was kicked back down to the lower court, we actually filed to have the case against us move forward. This allowed us to finally publicly answer the initial complaint, which I will share the most salient parts of, below:
That the decedent, Mona Haddad, had a history of depression since age 5
and had chronic suicidal ideation and attempts since age 7, with multiple suicide
attempts, as well as post-traumatic stress disorder (PTSD) related to childhood
trauma/neglect, with hot liquid poured down her throat by her mother; at age 15 and 16,
often being beaten with a belt by her mother who told her: "I wish you had never been
born". The diagnosis of borderline personality disorder was made during her
adolescence and during that time she was in a specialized residential program at McLean
Hospital for girls with borderline personality, followed by treatment in the Gunderson
Residence and Borderline Personality care continuum for adults with borderline
personality disorder.
In addition, as a result of the chronic threats to take her own life, many
psychiatrists and therapists refused to treat her. Further, as a result of her constant calls
and texts to members of her treatment team many times during the day and night, mental
health clinicians who treated her declined to treat her further, often sending her to
emergency rooms or inpatient psychiatric units to task teams at these higher levels of care
with finding new outpatient treaters for her. This was actually how Dr. MacMillan first
began her work with Mona when she was assigned her case while an inpatient attending
on the Trauma and Dissociative Unit at McLean Mona was clear that further terminations
of care by clinicians would lead to her death by suicide and so Dr. MacMillan felt
compelled and committed to continue working with her for as long as Mona wanted and
needed.
AS AND FOR A THIRD AFFIRMATIVE DEFENSE
172. After at least fifteen hospitalizations including multiple extended private
pay residential stays, including nine hospitalizations at McLean Psychiatric Hospital in
Massachusetts where she was confined for chronic suicide attempts, her parents were
told by the director of the Adult Borderline Center and Training Institute there, that they
should prepare themselves for Mona's eventual suicide. In addition, a well-respected
expert suicidologist at McLean did a consult on Mona when she was 18, several years
before she had met Dr. MacMillan or Dr. Muir, and commented in his report that
“Mona’s lifelong suicidality can be related to her mother’s chronic excitable state, and her
incapacity not only to quiet down her child, but to quiet down herself” and that “I regret
to say that the future risk of suicide for this very worthwhile and pleasant young woman
is extremely high.”
The strange relationship between Mona and her mother was a consequence of this
behavior of the mother and the reason for Mona’s statements in the Healthcare Proxy.
AS AND FOR A FOURTH AFFIRMATIVE DEFENSE
173. Mona Haddad was traumatized during hospitalizations by being
restrained in leather and soft restraints, being given medications over objection by
injections, and being isolated in restraint and seclusion rooms on 1:1 observation. On one
occasion, after overdosing on her medications, she was transferred to New York
Presbyterian Hospital for immediate medical stabilization, where, while being restrained,
in a delirious condition, she bit a nurse. who brought criminal charges against her.
Although, following her arrest, the charges eventually were dropped due to the nurse
not showing for the court appearance, the episode severely aggravated Mona's post-
traumatic stress disorder and suicidality. Consistently thereafter, Mona Haddad stated
that, “If I were ever hospitalized again, I will commit suicide.”
AS AND FOR A FIFTH AFFIRMATIVE DEFENSE
174. Throughout her course of treatment by many mental health clinicians,
Mona continued her constant threats of suicide, almost daily, with statements: "I need to
die". This was a compulsion characterized by the incessant need for reassurance from
others to manage these intrusive thoughts, a form of OCD known symptoms as "harm
OCD”, even though she did not actually want to die. When she ultimately came under
the care of Owen Muir, M.D. and Carlene MacMillan, board-certified psychiatrists with
specialized training and experience in treating complex patients like Mona, they
diagnosed Mona with severe obsessive compulsive disorder, characterized by symptoms
such as harm OCD about suicide, contamination concerns such as “pizza that touched air
that touched other pizza,” protracted rituals to leave the house, intense fears of fluids and
residues necessitating the use of multiple pairs of gloves and avoidance of physical
intimacy, health illness anxiety/hypochondriasis, as well as moral scrupulosity with
fears that she might be a “secret psychopath” or serial killer. Like many with OCD, she
had a relentless pattern of reassurance-seeking from clinicians, friends, family and even
specific suicide hotline workers to gain external reassurance that her many fears were
unfounded. By way of example, something as mundane as having a mild cold was
experienced as a possible terminal illness and therefore justification for suicide. Dr. Muir
treated Mona with "medication management". His partner, Carlene MacMillan, M.D.,
who, like Dr.Muir, has specialized training in an evidence-based therapy called
Mentalization Based Treatment for transdiagnostic and complex individuals with
personality disorders and trauma,, undertook to treat Mona as her primary therapist,
with Mentalization Based Therapy. Additional treatment was furnished by Robert
McMullen, M.D., an interventional psychiatrist in private practice who treated her with
deep Transcranial Magnetic Stimulation for Obsessive-Compulsive disorder and
Treatment Resistant Depression. In addition, Rebecca Berry, a clinical psychologist at
New York University Langone Child Study Center, treated this patient's obsessive-
compulsive disorder typically two times a week with specialized Exposure and Response
Prevention therapy at that institution. Dr. Berry had recently gone on maternity leave in
the month prior to Mona’s death. Mona was also a member of a Young Adult group at
the NYU Child Study Center at the time of her death.
AS AND FOR A SIXTH AFFIRMATIVE DEFENSE
175. For the one year of treatment during 2015 and 2016, by reason of the
comprehensive, collaborative and evidence-based treatment referred to above, Mona
Haddad improved significantly, so that during that year, she made a trip to Israel by
herself for Birth Right; visited her maternal grandmother overseas; connected with
extended family members on the Jersey Shore, moved into her own apartment; took
classes at Hunter College, where she received excellent grades; sang in a prestigious
choir; worked with children as a babysitter; volunteered as an activist and was in the
process of applying to college. In addition, she began dating and was creating and
sharing non-fiction creative writing pieces as part of processing her traumatic experiences
in childhood and in psychiatric hospitals and residential programs.
AS AND FOR A SEVENTH AFFIRMATIVE DEFENSE
176. Mona improved, as stated above, but continued to have high levels of
chronic and intermittently more acute suicidality. As she had with prior clinicians, she
called Dr. MacMillan and Dr. Muir from rooftops and train platforms at unspecified
locations, rehearsing suicide attempts. However, these calls from these types of locations
become less frequent over time. She ingested a potentially lethal amount of Prazosin and
immediately sought rescue. She hoarded a massive bottle of Tylenol but agreed to bring
it in for disposal. Her lifelong practice of constant suicide attempts and rehearsals, with
many threats of suicide, placed her at a high risk, when it came to the capability to carry
out a suicide attempt, regardless of the treatment setting. This, in addition to the nearly
nightly threats of suicide and self-abuse, delivered by phone calls and texts at all hours
to members of her treatment team made her prognosis quite guarded.
In close collaboration with Dr. Berry, her OCD therapist, Dr. MacMillan and Dr.
Muir attempted to put limits on her excessive reassurance-seeking behavior and created
realistic boundaries, to allow her to engage more productive out of session contact over
time. This included asking the patient to employ the practice of "scripting", before calling,
since the treaters reached the conclusion that taking her constant phone calls where she
would say: "I have to die", would perpetuate her severe OCD and be counter productive.
Prior clinicians often fell into a trap of initially allowing unlimited intersession contact
and when they realized that much contact was unsustainable and unhelpful, they would
impose strict contracts around no out of session contact and to call 911 if having an
emergency. Mona was unable and often unwilling to adhere to these contracts so
clinicians would terminate care, and she would end up in the hospital again. Dr.
MacMillan, Dr. Muir, and Dr. Berry’s stepped approach which was grounded in
extensively studied principles of cognitive behavior therapy, including exposure and
response prevention and dialectical behavior therapy, was resulting in an overall
trajectory of more appropriate and productive use of out-of-session contact. Her family
had been repeatedly informed and provided psychoeducation about this approach and
were in full agreement with it.
AS AND FOR AN EIGHTH AFFIRMATIVE DEFENSE
177. Mona Haddad's post-traumatic stress disorder, with repeated confinement
to psychiatric hospitals, made them extremely negative environments for her. Mona
referred to these confinements in an email, as follows: "I am afraid they are going to hurt
me. They are scary things. I am never going to the ER again."
Neither Mona nor her parents wanted her committed to a state hospital, nor
admitted involuntarily to Bellevue Hospital. It was clear that, in terms of meaningfully
modifying her risk of completed suicide, hospitalization was and would be
counterproductive. Mona referred to hospitalization as "punishment.” Furthermore
treatments that have strong evidence of treating suicidality, including Mentalization
Based Treatment, deep Transcranial Magnetic Stimulation, were not available in
inpatient hospitals accessible to Mona in 2016. There are no modifiable risk factors that a
psychiatric hospitalization would mitigate in Mona’s case but there were tangible risks
to hospitalization for her regarding re-traumatization, potential further criminal charges
and disruption to the positive activities and relationships she had been increasingly
engaged in while working with her outpatient treatment team.
178. When Mona Haddad was in the office of Owen Muir, M.D. on September
10, 2016, she immediately entered into an enraged state as she had learned from an
acquaintance that her mother had referred the acquaintance to treatment with Drs.
MacMillan and Muir. She was livid that he was refusing to disclose information about
the patient or agree to change any plans around what patients he sees in response to
demands and threats from her. When her dysregulated behavior quickly escalated to the
point where she was dramatically but implausibly attempting to hang herself with a cord
in the office, head-banging against a brick wall and screaming about the situation about
her mom referring the acquaintance, Dr. Muir had no choice but to tell her he would need
to call 911 if she did not stop the unsafe behaviors. She then coldly told Dr. Muir that "If
you call the police, I’m going to scream that you raped me" in hopes this baseless
accusation would deter him from calling and she could continue her inappropriate
behavior. While on the phone with 911, Mona did scream out what she threatened and
Dr. Muir calmly pointed out to the dispatcher she was screaming that he had raped her
in hopes he would hang up. This event was extensively documented by Dr. Muir in his
office records and is the only place where any mention of rape between Mona and Dr.
Muir was ever mentioned. It was never brought up again and instead Mona continued
to message both doctors about her anger and resentment regarding the acquaintance her
mother had referred, believing it was done intentionally by her estranged mother in order
to insert herself into Mona’s life yet again against Mona’s expressed wishes.
179. Mona Haddad was brought to the Emergency Room of New York
University Langone Hospital by her father, on the advice of Owen Muir, M.D. and
Carlene MacMillan, M.D. on September 24, 2016. Neither the patient nor the father
wanted Mona to be admitted but agreed she needed to be evaluated at a higher level of
care. If her condition required admission to the hospital against her wishes, under those
circumstances, it would have had to be Bellevue Hospital, since NYU Langone Hospital's
locked psychiatric unit is only for voluntary admissions. The next day, a plan was
eventually formulated by medical staff at New York University Hospital working in the
emergency room, and the plan was discussed with Dr. Muir, Alan Haddad, the father of
the patient who was present at the bedside, and Mona. The plan was to discharge Mona
that day and Dr. MacMillan had arranged for the initiation of IV Ketamine for suicidal
ideation at the private practice of Dr. Amanda Itzkoff to be moved to the following
morning rather than later in the week, as previously planned. The plan included the
stipulation that her father would go with her to her apartment, and he would remove all
lethal means to reduce the risk she would die by suicide that evening or following
morning and that he would accompany her to the Ketamine appointment in the morning.
This plan was agreed to by Mona and her father. Mona was discharged in the
company of her father. Mr. Haddad did not follow that plan.
The address was “eat———@fuckyou.com” which, in fairness, is a domain I would kill for.
I know this because, in keeping with the law after the Tarisoff decision which created “a duty to warn,” I received a phone call from that patient’s current treating physician, informing me of the patient’s intent to to end my life. This call was prior to that former patient being transferred to a psychiatric ER, evaluated, and subsequently discharged that night despite threatening to murder me.
Keep in mind, this is someone who wanted to end my life in the context of my having seen them a three (3) times in a community clinic. On one of those three occasions, I prescribed a generic non-controlled medication that I discontinued in consultation with that patient one week later.
This was cited as the cause of his intent to murder me. However, it is still an open question as to whether they were the only person at fuckyou.com who took issue some issues with me. The uncertainty is due to the following: I received a second aggrieved email, which was reportedly from f——-@fuckyou.com. It is not clear whether eatmy—- or f——— is in a managerial or executive role. I expect they keep it rather loose over at fuckyou.com? I hope this true life story provides helpful context when evaluating the Yelp reviews of physicians.
That young man is now a friend, and he’s also going to train in child and adolescent psychiatry. He heard me on clubhouse over a year ago, and it was life-changing for him. Disclosure like this is something I’ve become a strong advocate of, and it’s heartening to see colleagues following suit.
As first reported in whimsical fashion.
Rapid remission of suicidal depression in a day with brain stimulation. This paper was submitted for publication before there was even a name for this protocol, independently worked out and subsequently standardized by both Nolan Williams, M.D. and the team at my former practice and research site. His laboratory at Stanford went on to not only complete the most remarkable randomized controlled trial work on this treatment, but turn that approach into a patentable technology which is now being brought to market by Magnus Medical.
The SNT randomized controlled trial as published by Eleanor Cole and colleagues. I have talked about this before, but the ability to get suicidal depression into remission, even when refractory at prior treatments, in only five days, is the biggest news in medicine In my life.
The FDA breakthrough device program is blowing up.
Like being part of the clubhouse creator first program!
Like being part of the clubhouse creator first program!
I would appreciate it if no one clicked on the next link, but it’s just not practical. So here it is. Do with it as you will.
The Inferno, by Dante Alighieri, Canto III. No, you have not read that translation before, it’s mine personally. Yes, from the original Italian. Yes, I learned Italian only for the purpose of translations of Dante to English. What are you looking at? Unlike poet laureates like Robert Pinsky, whose translation I consider definitive, poetic translations will not be my life‘s best work (SM).
Intellectual Property. We call at IP. By the way, the We I am referring to there, in that sentence, is not the royal We. I mean those of us, so many, who have had to labor away in obscure health-tech start-ups, with the scant—but still precious!— the hope of acquisition by United before the real work can begin. That hope is the oxygen we breathe.
In what I consider to be an HR landmine…
Of course, I’m sure there would never be any such thing as discrimination in a company the size of UnitedHealth Group, particularly not based on disability, but for the education of all who are interested in employment law, particularly that in New York City as it applies to disability discrimination claims:
As of February 8, 2020, New York State law prohibits all employers, regardless of size, from making hiring, firing or other employment decisions based on disability if you are qualified for the job. Before then, New York State law applied to employers with four or more employees. Also, as of October 11, 2019, the protections against disability discrimination in New York State apply to independent contractors.
New York City law prohibits employers with four or more employees from making hiring, firing or any other employment decisions based on disability if you are qualified for the job. As of January 11, 2020, the protections against disability discrimination in New York City apply to independent contractors.
Under the disability discrimination laws, if you are qualified and able to do a job, an employer may not consider your disability when deciding to hire, fire, pay, give job assignments, promote, lay off, train, change benefits, or affect any other condition of employment. The laws define what a disability is in different ways. The types of disabilities generally covered under the ADA, for instance, include any impairment that limits a major life activity, like: hearing, seeing, speaking, walking, breathing, doing manual tasks and learning. New York State and New York City human rights laws cover additional types of disabilities, so more types of impairments are covered and more people are protected.
Your employer must generally make reasonable accommodations for your disability, unless your employer can show that the changes would be too hard or expensive for the company. Reasonable accommodations can include giving you special equipment or modifying equipment, devices, exams, training materials, work schedules, job assignments, company policies, and even changing your work station or work location to help you perform your duties.
Each case is different. Whether you are the victim of disability discrimination depends on the facts of your case.
Again, I think it’s pretty clear that deliberate indifference is a defense in the case of discrimination claims, and it has not been adjudicated otherwise. As an aside, can you imagine the legal lift of trying to demonstrate that something was too expensive for United with their $2 billion in monthly free cash flow?
And now, I am absolutely sure, as everyone reading this can completely tell, that nothing United or any of the subsidiaries of UnitedHealth Group would ever do could skirt anywhere close to regulations with which they would not be completely compliant, but just for the purposes of education, here is the definition of retaliation on employment law in the city of New York😍: (thanks: https://www.nycbar.org/get-legal-help/article/employment-and-labor/disability-discrimination/?amp).
Retaliation:
Retaliation occurs when you get punished by your employer because you exercised your legal rights or because you engaged in a lawful activity. Federal, New York State, and New York City law make it illegal to retaliate against employees for:
Reporting or filing a discrimination claim or a sexual harassment claim;
Participating in an investigation or a lawsuit about a claim (even if it is decided that your employer did not do anything wrong); or
Retaliation can occur in any aspect of employment, including:
Hiring, firing and layoffs;
Pay and fringe benefits;
Job assignments, promotions and training; or
Any other term or condition of employment.
Retaliation can be obvious, but it can also be so unclear that you do not notice it until long after it occurred. If you have experienced any of the following, you may be a victim of retaliation:
You report your employer to officials for unlawfully not paying overtime; soon after, you are fired.
You cooperate in an investigation into whether your employer unlawfully failed to pay minimum wage and overtime… and you are not offered any promotions.
You have always received great job performance reviews. Then you reported to your human resources department that a co-worker (a rising star at that!) was sexually harassing the women he worked with…
You lawfully take time off to care for a sick relative; when you return to work, you are the only employee who does not receive a raise for the next year.
You testify in a race discrimination lawsuit against your employer. Then you are transferred to the night shift.
I’m sure my relentless advocacy for mental health parity—including having personally taken United to court, or reporting them repeatedly to the Attorney General of the State for denials of care in violation of generally accepted standards and won—does not fall into this same category in any way, shape, or form.
Like this:
It’s not like having a systematic approach to collecting information about disability status prior to summarily dismissing applicants gives rise to any liability whatsoever for the mega-corporation in question. Because it’s not like they essentially automatically generated a class that could take legal action of any kind? I mean, what would we even call that kind of lawsuit? I’m sure there is a paper trail that documents that every single person rejected from this application process was done because they didn’t qualify for any of the jobs so it couldn’t possibly be asserted that this is due to systematic discrimination against people who voluntarily disclosed disabilities! Or those, like myself, who have successfully advocated against their hegemony in violating mental health parity law? Nor their capricious ERISA violations related to network insufficiency as defined under the ACA and, which as of 2021 Combined Appropriations Act, were also fiduciary breaches on the part of brokers and employers selling any UHC products in NYS and NYC at a minimum?
Linguistic pro tip: anything you say before the word ”but” will be interpreted as dismissed by anything that follows it.
Starting with a patent application or intellectual property filing for that extremely valuable piece of IP gold. Your Life’s Second Best Work (SM) has a real ring to it!
The inspiration for our humble narrator, O. Scott Muir, M.D.
It’s the only way it generates more profits. So getting sued drives up costs, and in this very strange context, that’s how United becomes more profitable!
Hi!