


What is "Adult ADHD"?
A child and adult psychiatrist--with ADHD-- explains what you need to know.

Attention-Deficit/Hyperactivity Disorder (ADHD) is something I see regularly in both children and adults. This article is a “re-run”—but some questions about this popped up on a listserv I participate in, and thought it might be helpful to re-share.
The following article is referenced extensively, and should prove a helpful guide. We will learn:
What is ADHD?
What are the problems with the diagnostic process for ADHD?
Do you need fancy testing to tell?
Does psychotherapy help for ADHD?
What biological treatments exist for ADHD?
What’s the deal with stimulants?
Do we need to be terrified of dangerous controlled substances?
What else works?
I will begin by establishing up my credentials to speak about the topic, because a lot of fakers have opinions, and it's hard to know what to make of them. I am dual board certified in general and child and adolescent psychiatry.1

ADHD is included in the Diagnostic and Statistical Manual for Mental Disorders. I’m on a committee for continuing medical education created by the American Academy of Child and Adolescent Psychiatry (AACAP). We make the “Clinical Essentials” trainings through AACAP, and I have the pleasure of narrating the official training on ADHD through that professional society!
My wife, and sometimes coauthor, Carlene MacMillan, M.D. is the chair of the AACAP consumer issues committee, who created this official ADHD resource center for families.
I also, as a human, have ADHD myself.
If that isn’t “rolling deep” on ADHD and it’s treatment, to you as a reader, I never want to meet you in the back alley of an academic medical conference. I'm pretty sure I'll get my ass kicked by someone with more ADHD credibility. You know, because the multifactorial relationship between impulsivity and violence in people with ADHD.
Originally understood as a disorder of childhood, it persists into adulthood with varying degrees of impact and impairment. ADHD has a long history.
My Opinion:
I don’t necessarily consider it a “disorder” in the most common sense of the word":
It’s a disorder in the same way being tall is a disorder in a world with only too-short doors. The population prevalence is around 10%. In evolutionary terms, anything that's that common can't be something that bad for your species.
I think it's fair to say that the treatment of ADHD has been in the news…
What is Adult ADHD?
My working definition is that, for Adults, ADHD is a primarily a context-dependent difference in how attention is allocated. It also has other emotional and behavioral consequences, but this gives us a place to start.
Adults with ADHD have trouble paying attention to things they find boring. However, they are exceptionally good at paying attention to things they find interesting. We like novelty (stuff that’s new or different), more than most. Adults with ADHD also tend to be good at tasks that require hyper-focus. This is zooming in with our attention on one particularly interesting thing. It’s a state of such focus that it leads to the exclusion of other input from their surroundings.
Evolutionary biology can help us think about it:
It was good to have a few distractible hunters around. We were in tribes on the Serengeti. A few tribes-people poking around meant extra gazelles for dinner. While most individuals would be looking ahead at the main hunt, a few distractible outliers means everyone ate more at the meal. This is a life and death difference, and we are the result of how much better it was to have that variation in our ancestors.
In the context of having to sit in school—or worse, paying attention on Zoom—the same ability to be distractible becomes a disability. Imagine an allergy to boredom. Some people have just a little itch with their allergies. Some can die from abrupt and extreme anaphylaxis. ADHD is, in part, an allergy to things that are “boring” according to that person’s brain.
Just like allergies, the range of experience with ADHD is broad. Some people have just a touch of “the inattention.” Others will avoid tasks that require attention (e.g. tax preparation and editing this very substack for sentence structure) like a bee sting to the deathly allergic. People don’t get a list in advance of plausibly boring things and get to choose what they will hate. They don’t get to pick VERY ENGAGING. It’s just assigned to each person, thank to the fates. And they have to choose what to do with it. Like Stan Lee’s X-Men—mutants who had super powers and terrible curses—it is finding the right context and the right community that made being a creepy looking beast into a world saving super hero. So, too, ADHD is often about what you do with it.
My Opinion:
ADHD is a brain difference. Sometimes it's a problem. Sometimes we can help. There's nothing wrong with you, in the bad sense of the term “wrong.” Sometimes the environment and the person aren't the best fit. If we can help, there are benefits to doing so, and risks.
The Muir-Cox Criteria for ADHD
Lara Cox, M.D. is a remarkable physician with whom I trained. She also has ADHD, and taught me a heck of a lot about it. Together, as a joke, we developed a set a four criteria that she believed were much faster screening questions for ADHD than a traditional symptoms of inattentive-type ADHD. In over 60,000+ hours of clinical practice, my experience has been that these questions are a reliable predictor of having all nine out of nine inattentive symptoms of ADHD as taken from the DSM-5.
The four questions are as follows:
What happens when you try to meditate?
Do you worry that you're lazy or dumb?
Do you procrastinate?
Are you less good at things than your level of smart would predict?
The questions aren't intended to be elegant. But there is a pattern of responses to them, which I will share now, which are the “positive” findings.
Q: What happens when you try to meditate?
A: Answers to this question are often “you're kidding right??” Or in the realm of incredulity that anybody could do any meditation. The ability to empty one's mind is some thing that is almost unimaginable to people with ADHD coming to see a psychiatrist, and so it's really the emotional reaction as to the impossibility of meditation that I'm looking for. It's worth noting that experienced meditators often grappled with these questions in meaningful ways, and so this is more of a question for general audiences.
Q: Do you worry you're lazy or dumb?
A: Self-reproach for not being good enough is often internalized by people with ADHD. Because it's not obvious to any of us what our brains are preventing us from doing, there are often important tasks that people with ADHD find themselves avoiding for unclear reasons so the default is to think one is lazy or dumb. This avoidance is what the question is getting at. And if you ask it this way, it often reveals itself under a layer of casual blame of the self.
Q: Do you procrastinate?
A: The answer to this is usually a shared laugh, based on what they've told me already. Procrastination, which is the “avoidance of tasks that require sustained mental effort” for “boring” things is a key feature of inattentive type ADHD. This is often a moment of humor in a psychiatric interview.
Q: Are you less good at things than your level of smartness would predict?
A: The speed with which this question is answered with a loud YES is what tends to stand out. It's phrased in this awkward way on purpose. This is so people will ask questions about what I mean. It’s also so awkward, in wording, that inattentive people will miss it. This is also diagnostic info for me, at 60K+ hours of pattern recognition asking the same questions.
It's often smart people who underperform. This is especially common in women. Because the hyperactive symptoms of ADHD are less common and girls and women, they don't cause trouble in the classroom early on. They are commonly “missed” when they are young girls when it comes to an ADHD diagnosis.
The under performance is due to the ADHD-unfriendly constraints—distractions, timed conditions—of what they had to complete in school or work.
It's a little bit like asking people about their beekeeping skills when they have a deathly allergy to bee stings. Those individuals are likely to underperform at beekeeping, no matter how good they have the potential to be at the basic bee-maintenance skills that go into it.
My Opinion:
This is an approach for experts, and one that is intended to be lighthearted and make a clinical interview a little easier. That having been said, according to the American Academy of Family Practitioners, the evidence for rating scales and screening measures is bad—a “C” rating indicates that the evidence is not strong. It's an empirical question as to whether even goofy questions like the above are better or worse than our current standards2. We need to do better.
It’s Not Anxiety…Sometimes It’s ADHD.
Adult ADHD can often feel like anxiety for people with ADHD, particularly when their energy levels are low, their attention spans are strained, and their environments are disorganized.
I will often ask my patients if they feel anxious coming home at the end of the day? I will then follow up with: “does it have to do with things like cluttered surfaces or a messy coffee table?”
My patients with ADHD will say, “Of course! I have to clean it off entirely.” The chaos on the coffee table is a reflection of the chaos in the person’s mind. The experience of the disorganization causes distress and agitation. I don’t understand this same brain circuity as “generalized anxiety disorder” or other anxiety disorders, although they can overlap.
What makes adult ADHD different from a generalized anxiety disorder is that it’s the clutter, chaos, and disorganization that gets in the way of focusing— not worrying about intrusive anxious thoughts about past performance or future woes.
The Process of ADHD Diagnosis and its Discontents.
ADHD is a condition that is currently diagnosed clinically. This means the diagnosis is based on history and examination, not neuropsychiatric testing.3
History: the story a patient tells you.
Examination: what you observe while they tell that story.
There is no definitive required testing to make an ADHD diagnosis! An ADHD diagnosis is made by a mental health professional with the expertise to navigate the process of a differential diagnosis. The role of neuropsychiatric testing is to answer questions that are not answerable from that history and examination. I can't tell, just by talking to someone, if they have a specific deficit in working memory, reading comprehension, or other measurable but subtle cognitive functions.
The question, in any diagnostic interview, is why. What is the best explanation for: 1. the story I've been told and 2. the observations I'm making? People come to see me with complaints of inattention, underperformance, distress, or those problems along with their “presenting complaint.” Our task is trying to parse out why. Attention is a process that involves myriad brain networks. It’s complicated. We don’t want to mistake it for something else. Often, people have more than one DSM-defined problem. Difficulty paying attention may have to do with the fact that you're traumatized, depressed, or have ADHD, and sometimes all at the same time.
My Opinion:
Not all inattention is ADHD, and not all ADHD is inattentive. It's important to understand the difference.
Do we need neuropsychologic testing?
Neuropsychologic testing is a lot like an EKG for a heart condition. You can tell with your stethoscope if a person has a heartbeat that's skipping, but you can't tell electrophysiologically why. So you get more testing. When it comes to ADHD this is called neuropsychologic testing. The difficulty is of course this testing is usually very expensive, often comes with long wait lists and takes a lot of time.
For my colleagues in industry, the ability to create more reliable diagnostic tools for ADHD would be a godsend. It's a complex condition, but we don't have the kind of biomarkers yet that we do for heart disease. It would be awesome if we could define digital phenotypes for ADHD and integrate those into our clinical and diagnostic digital toolkit. #FreeStartUpIdea.
What About Therapy?
Psychotherapy has been turned into the branded product: “Therapy” by venture backed companies. Just ask Michael Phelps:
It's not that simple. We have an evidence base for psychotherapies, plural, for a variety of well-defined conditions. Is there a specific therapeutic modality that is helpful for the underlying condition we are talking about?4
When it comes to attention deficit hyperactivity disorder, I've got good news and I've got bad news about therapy.
The bad news, first:
There is no standalone psychotherapy that is as broadly effective for ADHD as the medications on the market today. As covered in my prior articles, the most definitive RCT on this is the MTA study5, done at NYU among other sites. In this study, psychotherapy and methylphenidate were compared in children. The study was stopped early by the institutional review board. Methylphenidate, a kind of stimulant medication, was so much more effective than psychotherapy that it was considered unethical to continue to prescribe placebo to children and just give them therapy.
The good news:
There is one specific therapy, organizational skills training6, or OST, which is effective for executive dysfunction and ADHD. This therapy is not widely available, many therapists are not trained on it and I am highly skeptical any of those therapists are who you will match with on Talkspace.
People with ADHD often have other problems7, and therapy may be helpful for those other problems. Therapy can also be helpful to cope with or understand what it’s like to live with ADHD, especially if you have felt or been told you are stupid and/or lazy for much of your life.
Psychotherapy is NOT an effective treatment for the core symptoms of inattention or hyperactivity.
One of the reasons ADHD is also so justly in the house of medicine, is that it requires parsing out other problems in the body that can be mistaken for ADHD:
Problems or conditions that can “mimic” ADHD, or make it worse8
… and so much more. ADHD is a medical condition. It most commonly presents in childhood, but many people are not diagnosed then. The first line treatments are stimulant medications, but these aren’t right for everyone.
My opinion:
Differential diagnosis for adults with attention problem is complicated, and that's what requires the time. We don't have great tools to diagnose ADHD itself, but we have appropriate tools to diagnose all the other things that can be confused with it. And we should use them.
Promising novel treatments being researched include transcranial magnetic stimulation (TMS), recently FDA approved monarch eTNS device, and LSD derivatives, now in clinical trials, with Mind Medicine9 as the industry sponsor, and more.
My Opinion:
The next generation of treatments are exciting. They promise better efficacy and a lower side effect profile. And that's what we need.
Thinking About Treatment With Stimulant Medications?
Stimulant medications are a first-line treatment.
There are two major classes of stimulants, and these are amphetamine salts and methylphenidate. Adderall and Ritalin are two brand names of compounds developed in these two classes. Similar compounds that are legally still prescribed— but very rarely are chosen because of the higher risks— include dexedrine and methamphetamine. For very good reasons methamphetamine is not the kind of thing that is routinely prescribed for ADHD.
There are short acting stimulants, and there are long acting stimulants. There are a variety of different formulations of long acting stimulants.
Stimulant medications work because they provide more dopamine in the prefrontal cortex (the part of the brain that does “wait, hold on one moment!” thinking…) as pictured here:

And more specifically, here:
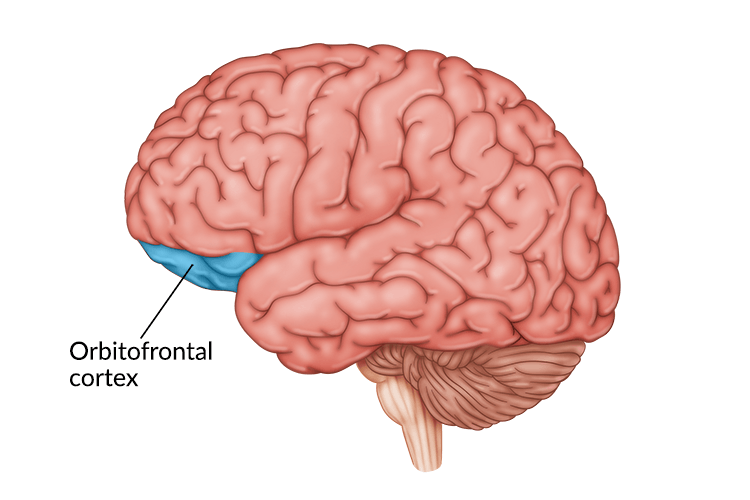
Orbitofrontal= just above above the eyes!
That’s where the focus promoting effects of the medication are are acting. Since these drugs are blunt instruments when it comes to dopamine released, dopamine is also released in other pathways in the brain, including the nucleus accumbens (a tiny area pictured here):
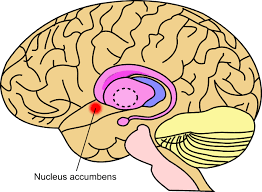
…which is part of the reward circuitry of the brain. It is strongly implicated in addiction to the euphoric properties of stimulant medications.
In individuals with ADHD, they don’t actually get the same euphoric effect from dopamine increasing stimulants, or at least not at the dosages that we are using for treatment. They have a lower “dopaminergic tone” in their brain which certainly contributes to all that novelty seeking they are known for. The ADHD brain is less sensitive to dopamine—they don’t generally get the same “high” from the same dose of medication as a non-ADHD brain. Very strong biases in these data is that most of it is from college students, many of whom like to get high.
The reasons why prescription stimulants are misused are numerous and include achieving euphoria, and helping cope with stressful factors related to their educational environment. According to a survey of 334 ADHD-diagnosed college students taking prescription stimulants, 25% misused their own prescription medications to get “high” (Upadhyaya et al. 2005).
Given the rates of cannabis and alcohol use among college students to get high is around 50%, the above number is actually low compared to the base rate of getting high with other things.
My Opinion:
Addiction is a real problem for some people and people with ADHD are suffering nonetheless. It deserves to be treated appropriately, and that means to not shy away from the most effective treatment that exists.
Broad Strokes, People: Benefits of Treatment of ADHD.
In people who don’t have ADHD, you get about a 30% performance boost from taking stimulant medication. People with ADHD, on the other hand, get a more significant boost in performance. It's a 17% boost an academic scores, which is between two and three letter grades better. It's a huge deal. These kinds of improvements change life trajectories. We base a lot of decisions at key moments in our development on the grades we got, and if you have ADHD, the data strongly supports the scores improving. This can be life-changing.
Stimulants are likely less addictive in people with ADHD if taken as prescribed, and more helpful in terms of improving performance, because they’re treating an underlying disorder, not just providing an “artificial” boost to performance. That artificial boost is real for others as well, but the risks and benefits don't have the same math.
People who are being treated for their ADHD are less likely to develop criminal behavior, which is a risk of untreated ADHD in youth. If you don’t believe me, go to literally any juvenile correction facility and spend 20 minutes there, and then tell me what you think. Or just read the following meta-analysis, and you'll see it's about 25% of that incarcerated youth.
It’s like the ICU for ADHD, but unfortunately, only after the justice system has taken a crack at ruining your future, and the future of your children.
My Opinion:
Abolish imprisonment. It's a pox on the house of human decency and we should be ashamed of our behavior as a society. But that’s for another substack post…
Additionally, people with ADHD who have treatment are less likely to develop addiction as well. The fewer the ADHD symptoms someone is struggling with thanks to early treatment, the less likely they are to develop a substance use disorder. Paradoxically, oftentimes it is precisely these individuals who are most vulnerable to addiction who are turned away from getting this effective treatment or whose parents think it is contraindicated so never even explore the possibility.
My Opinion:
Stimulants are remarkably effective. So is fire, both to keep you warm and burn down your house. We need to be careful, but we can't live in darkness.
Other Medication Options
Cochrane does reviews of the evidence across medicine. Thank God, says every doctor in training, for the Cochrane network’s meta-analyses. Now I have something to say on rounds when asked!
They reviewed alpha agonists—medications like clonidine and guanfacine— in ADHD. But, it’s been more than four years, so they pulled the publication. Can you tell we need more research?
A 2013 review, that hasn’t pulled for being too dated, stated the following:
Clonidine and guanfacine have been shown to be effective for the treatment of hyperactivity, impulsiveness, and inattention across several studies. After nearly three decades of experience with clonidine, its advantages and disadvantages are well known. While support remains sparse for immediate release guanfacine as an efficacious treatment for ADHD, substantial evidence demonstrates the efficacy of extended release guanfacine in the treatment of children with ADHD. In 2009, Intuniv® (guanfacine XR) was the first among alpha 2 agents to be FDA approved for use for treatment of ADHD in children and adolescents. In addition, a long-acting form of clonidine, a frequently used alpha 2 agonist, is in the process of being developed for use in ADHD.
For me, in 2023, the above still holds. We need more evidence and novel treatments, and as you can see above, they're coming, but the awareness of what already exists is also important.
My Opinion:
Alpha-agonists are not as effective for inattention as stimulants. Not by a long shot. These are effective treatments and allow for lower cases of stimulant medication when prescribed alongside them in some cases, and should be considered more often. Specially in adults with hypertension, they do two good things for those individuals at once.
What about Strattera?
Atomoxetine is a non-stimulant medication, brand-name Strattera, that has decent evidence to support use in children when stimulants are not a good fit. There have been extensive reviews. However, it's data in adults is relatively weak:
Cunill et al completed a systematic review and meta-analysis on twelve randomized, controlled trials (3,375 subjects) comparing ATX to placebo in adults with ADHD.38 They calculated the standardized mean differences using clinician rated scales at −0.40 – a modest effect size. They noted that few subjects discontinued due to lack of efficacy (5% with ATX and 6% with placebo). However, a larger percentage of subjects discontinued because of adverse events (AEs) while taking ATX (13%) compared to 5% while on placebo. They concluded that the evidence to recommend ATX to treat ADHD in adults is weak because of the AE profile.
It works about half as well (0.4 vs 0.8-0.9 effect size) as stimulant medications. It’s not particularly tolerable for many.
My Opinion:
As much as we want something that's not a controlled substance to be a great treatment for ADHD, I can't say that atomoxetine is that something for most people.
In Summary
Attention deficit hyperactivity disorder is real. It starts in childhood. It persists into adulthood. It's a fundamental and common difference in how brains function. Sometimes it's helpful, other times it's not.
The most effective treatments, stimulants, have significant risks and downsides. They also work well for some of the core symptoms. We can't be terrified of them just because they're controlled substances. The role of professionals, particularly those with significant expertise, is to educate, not just to prescribe.
Other treatments exist:
Strattera isn't very good in adults. If it works for you, great, but the odds are less that it will work for many adults than stimulants.
Clonidine and guanfacine are pretty good at dealing with hyperactivity/impulsivity and improving treatment with stimulant medications that can in turn be given at lower dosages.
ADHD interacts with a bunch of other conditions, and the medical assessment of people with ADHD is important, because attention is such a broad brain function. Problems with attention might be an underlying medical problem raising its hand and ask to be noticed. Physicians can take better care of our patients and ourselves if we pay attention to attention.
Treatment for co-occurring medical conditions is crucially important.
Screening for autoimmune conditions, sleep disorders, addictive disorders, post infectious cognitive impairment, malnutrition, should be part of any comprehensive medical evaluation for adult ADHD. It's not just a checklist of symptoms, it's an assessment of how someone's brain is working, and why.
Thanks for joining me, I appreciate your time reading this article and sharing it with your friends. If it's helpful, please feel free to let me know that also. And I accept requests, if you have them. I'm happy to write more about what you're curious about from my perspective. This column , for example, was a request—I'm looking at you, fellow healthcare hacker!
—O. Scott Muir, M.D.
Here is the proof:
Adler LA, Faraone SV, Spencer TJ, et al. The reliability and validity of self- and investigator ratings of ADHD in adults. J Atten Disord. 2008;11(6):711-719.
Where I live, this testing can run into the thousands of dollars. It’s a major expense. And it’s not necessary for the diagnosis.
I'm not referring to eclectic or generic therapy to help you really make sense of your life, which is a worthwhile endeavor, but not a treatment for a specific medical condition.
The MTA Cooperative Group. A 14-Month Randomized Clinical Trial of Treatment Strategies for Attention-Deficit/Hyperactivity Disorder. Arch Gen Psychiatry. 1999;56(12):1073–1086. doi:10.1001/archpsyc.56.12.1073
The citation for the manual is as follows:
Gallagher, R., Abikoff, H. B., & Spira, E. G. (2014). Organizational skills training for children with ADHD: an empirically supported treatment. Guilford Publications.
Katzman MA, Bilkey TS, Chokka PR, Fallu A, Klassen LJ. Adult ADHD and comorbid disorders: clinical implications of a dimensional approach. BMC Psychiatry. 2017 Aug 22;17(1):302. doi: 10.1186/s12888-017-1463-3. PMID: 28830387; PMCID: PMC5567978.
Dear colleagues, you're welcome. It is a holiday literature review if ever there was one. I just learned a lot!
I am a shareholder, but not a large one. Conflict of interest disclosure:
…complete! How is that for transparency?
After being asked to do so by a conflict therapist, my brother just got an ADHD diagnosis this summer, at age 58. He has led a life full of conflict, with me and many others. He faced a staff rebellion at work and was reprimanded, was divorced and fired from his own book club. He is lonely and remains in a relationship with a woman who he says treats him poorly, for that reason.
Unfortunately, he also has built a bullet proof narrative that his behaviour isn't related to his isolation.
He manifests what seems like RSD. His brain instantly erases memories which reflect poorly on him, so he never learns from experiences. I am not qualified to know whether this is ADHD or deliberate cognitive dissonance management, but it is infuriating.
Bro tells himself that he has managed his ADHD really well. He even suspected during 6 years of therapy that he had ADHD, but he never investigated, because he didn't want to feel "more broken". He says his marriage was solid, despite ending in divorce and creating a very hostile former wife, because any other conclusion would be "devastating" to him.
Having recently received a long letter from him, quoting bible passages and insisting that I need to change, I find myself in a dilemma.
I have come to the point where I do not want more face to face contact with him, as long as he remains untreated, but I cannot oblige him to seek treatment. We do not live in the same city, so we do not run into each other. Although we can talk on the phone, our relationship doesn't work in person because of his low empathy, low self awareness and high impulsiveness.
I believe if I respond to him and make our relationship conditional on his getting treatment, which probably means medication, he is likely to respond with great anger and more biblical quotations about forgiveness, because he cannot accept responsibility for his behaviour.
Yet I do not want to just slink out of his life with no explanation, as he is my only brother.
This is how i felt about ADHD... before it became a crazy. Its almost become a culture bound syndrome. Now its literally every single adult intake who cant focus, maxes out ASRS scales and your questions, recalls "always" struggling with focus and attention. By the time these intakes get to psychiatry, they have thoroughly investigated the diagnosis. They know A LOT about it. Their memories start to get colored to reinforced their belief of having this diagosis. "I took a stimulant and it helped". I disagree people want to get "High". There are some who will abuse it. Id argue its more for (perceptions of) performance enhancement and energy. Even if you dont have ADHD and taking a stimulant - its going to make one FEEL that they are doing better. At least in the beginning until the tolerance kicks up.
Testing is another supportive feature to back up a dx instead of giving everyone who asks for stimulants stimulants. The truth is we weren't there in their childhood and have no idea how they functioned. It remains a neurodevelopemental diagnosis that CAN persist into adulthood. For those who do have missed ADHD diagnosis through adulthood, I do feel for because of all of the roadblocks, but its very unlikely to be every single intake. As below said, "Most people don't make til 45-50, and have successful life with adhd"
ADHD dx has unfortunately dichotomized into 1) What's the big deal, treat the inattention and give stimulants out. They aren't that bad. [...They're not?] 2) You can focus, you just don't want to and trained yourself not to. You don't need stimulants, you made it this far. You just need to change your behaviors [...Oh, wow okay thanks for the wake up call. So easy!].
We really need better guidelines here. Above is notorious in both psych and primary care. Without biomarkers, its hard to over/under diagnose, but I would argue its over treated. The more lenient we are with the diagnosis, the more right were going to move that 10% on the far end of the spectrum. Were going to have an entire country on stimulants (with a huge shortage as it is). As prescribers we became the gatekeepers of stimulants.