

Lithium: The Depressing Case of Misrepresented Monitoring Data III
Lithium: The Depressing Case of Misrepresented Monitoring Data III
Our guest epic on a remarkable medicine continues.


This is part three of a guest series— here on the internet’s leading health-themed daily-enough newsletter. He covered some of this as a guest writer on Psychiatry at the Margins in a previous guest post.
Remember, you can learn more about lithium by buying my book, Inessential Pharmacology. (amazon link). You can also catch up on
’s articles on lithium in part I and part II. Lithium has remarkable data. There has been excellent coverage in the Carlat Report on recent updates in lithium, like this one. Mood disorder experts and some humans coping with bipolar disorder alike appreciate Lithium. Alex attended a lecture by an “expert” in lithium dosing. He noticed a problem. So now a physicist has decided to present his counter-argument to the world, and The Frontier Psychiatrists is the platform. It’s no Stahl’s Guides, but it will have to do:“Multiple daily dosing distorts the level.”
The TL;DR? No, it does not. Not really.
It is the other way around. Single Daily Dosing (SDD) produces a “distorted” 12-hour lithium serum level. In my opinion, distorted is not the optimal word to use in this instance. I would say that SDD regimens, compared with their Multiple Daily Dose (MDD) counterparts, tend to produce a systematic error in the interpretation of the 12-hour level. In other words, there is often an offset between the observed 12-hour serum level value and the theoretical clinically useful 12-hour value.
The initial optimal reference ranges for the 12-hour serum level were mostly based on clinical observation and retrospective studies of patients on MDD regimens who responded and didn’t respond to treatment (and patients who became intoxicated) according to a 1980 paper by Amdi Amdisen [1], the researcher who developed the standardised1 12-hour level. Notably, the reference ranges did not apply to SDD regimens [2].
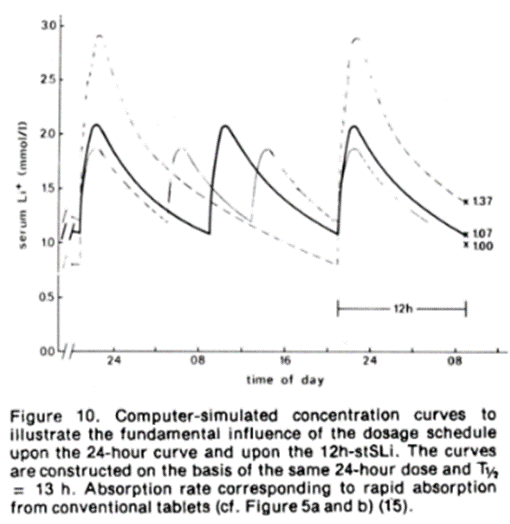
One of the reasons they weren’t applicable is alluded to by Dr Meyer in the quote from part 2. SDD regimens tend to give 12-hour levels around 10 – 30% higher than those on twice-daily dosing regimens [3] (and MDD regimens generally). This is illustrated in a computer simulation plot by Amdisen [2] for a theoretical patient with the same 24-hour dose and elimination half-life
There is some evidence that many psychiatrists are not taking this systematic error into account when interpreting patient 12-hour levels. According to Table 5 of the 2019 systematic review of optimal serum lithium levels by the ISBD/IGSLI task force [4]:
The recommendations for optimal serum lithium levels with once daily dosing of lithium should be the same as compared to twice daily dosing (endorsed by 90.9% [of the 33 Task Force members])
So now let us return to the paper by Castro et al. [5] that Dr Meyer references from part 2. It was a retrospective study, looking at “electronic health records from a large New England healthcare system between 2006 and 2013”. If we assume that most of the psychiatrists within the New England healthcare system did not differentiate interpretations of 12-hour levels between patients on twice daily dose and single daily dose regimens, patients who received a SDD regimen would have been on a lower mean serum concentration (Area under pharmacokinetic curve divided by time interval) than patients who received lithium twice a day (Averaged over the entire patient population).

Basically, in clinical practice, it is possible that patients on SDD regimens often receive less lithium than patients on MDD regimens.
There is precedent for this occurring. In the 1980s, Hetmar et al [6], [7], [8] observed the renal function of 46 patients after 10 years of lithium therapy. They found that urine volume was significantly higher and estimated Glomerular Filtration Rate (eGFR) significantly lower in patients receiving MDD compared to SDD regimens. However, as Carter et al. [9] comments:
Owing to the pharmacokinetics of the various regimens, patients in the MDD group were receiving higher lithium dosages to produce equivalent [12 hour lithium] serum levels.
Therefore, rather than determining risk between dosing regimens, is it simply the case that Castro et al. [5] showed that patients on a lower mean lithium serum concentration had less risk of developing renal problems? Well…
Stay tuned for part IV! Give
a subscription, too![1] A. Amdisen, “Serum Concentration and Clinical Supervision in Monitoring of Lithium Treatment,” Ther. Drug Monit., vol. 2, no. 1, p. 73, 1980, doi: 10.1097/00007691-198001000-00009.
[2] A. Amdisen, “Clinical and Serum-Level Monitoring in Lithium Therapy and Lithium Intoxication,” J. Anal. Toxicol., vol. 2, no. 5, pp. 193–202, Sep. 1978, doi: 10.1093/jat/2.5.193.
[3] D. Moscoso et al., “Lithium Therapeutic Drug Monitoring; Once Daily vs Twice Daily Dosing and the Impact of Renal Function,” 2020, Accessed: Aug. 11, 2023. [Online]. Available: https://tspace.library.utoronto.ca/handle/1807/101578
[4] W. A. Nolen et al., “What is the optimal serum level for lithium in the maintenance treatment of bipolar disorder? A systematic review and recommendations from the ISBD/IGSLI Task Force on treatment with lithium,” Bipolar Disord., vol. 21, no. 5, pp. 394–409, Aug. 2019, doi: 10.1111/bdi.12805.
[5] V. M. Castro et al., “Stratifying Risk for Renal Insufficiency Among Lithium-Treated Patients: An Electronic Health Record Study,” Neuropsychopharmacology, vol. 41, no. 4, Art. no. 4, Mar. 2016, doi: 10.1038/npp.2015.254.
[6] O. Hetmar, T. G. Bolwig, C. Brun, J. Ladefoged, S. Larsen, and O. J. Rafaelsen, “Lithium: long-term effects on the kidney I. Renal function in retrospect,” Acta Psychiatr. Scand., vol. 73, no. 5, pp. 574–581, 1986, doi: 10.1111/j.1600-0447.1986.tb02727.x.
[7] O. Hetmar, C. Brun, L. Clemmesen, J. Ladefoged, S. Larsen, and O. J. Rafaelsen, “Lithium: Long-term effects on the kidney—II. Structural changes,” J. Psychiatr. Res., vol. 21, no. 3, pp. 279–288, Jan. 1987, doi: 10.1016/0022-3956(87)90029-X.
[8] O. Hetmar, U. J. Povlsen, J. Ladefoged, and T. G. Bolwig, “Lithium: Long-Term Effects on the Kidney: A Prospective Follow-up Study Ten Years after Kidney Biopsy,” Br. J. Psychiatry, vol. 158, no. 1, pp. 53–58, Jan. 1991, doi: 10.1192/bjp.158.1.53.
[9] L. Carter, M. Zolezzi, and A. Lewczyk, “An updated review of the optimal lithium dosage regimen for renal protection,” Can. J. Psychiatry Rev. Can. Psychiatr., vol. 58, no. 10, pp. 595–600, Oct. 2013, doi: 10.1177/070674371305801009.
I told you, Alex is from the UK. This is how they spell it over there. -OM
 | A guest post by
|