



Geo— earth. Don—sounds like… down. To earth. Geo…Don. A drug name is born.
Welcome to the Frontier Psychiatrists newsletter. It is a leading health-satire-regulatory enthusiasm newsletter.
This article is another in my series about one drug or another. Prior installments include Ambien, Prozac, Xanax, Klonopin, Lurasidone, Olanzapine, Zulranolone, Benzos, Caffeine, Semeglutide, Lamotrigine, Cocaine, Xylazine, Lithium, dextromethorphan/bupropion and Adderall, etc.
Geodon: Drug, Interrupted.

Geodon—trade name, ziprasidone—is yet another “atypical antipsychotic” medicine. The other term is “second generation” antipsychotic. They have been growth products and profitable, if not so cost-effective1. Geodon has been only modestly effective in both bipolar illness and schizophrenia2. Here is what the FDA label says about Geodon:
GEODON is an atypical antipsychotic. In choosing among treatments, prescribers should be aware of the capacity of GEODON to prolong the QT interval and may consider the use of other drugs first (5.3)
GEODON is indicated as an oral formulation for the:• Treatment of schizophrenia. (1)
• Acute treatment as monotherapy of manic or mixed episodes associated with bipolar I disorder.
• Maintenance treatment of bipolar I disorder as an adjunct to lithium or valproate.
And Ladies, in Case You Were Wondering If Involuntary Intramuscular Injection Was an Option for Your Man, Geodon Won’t Disappoint!
GEODON as an intramuscular injection is indicated for the following:
• Acute treatment of agitation in schizophrenic patients.
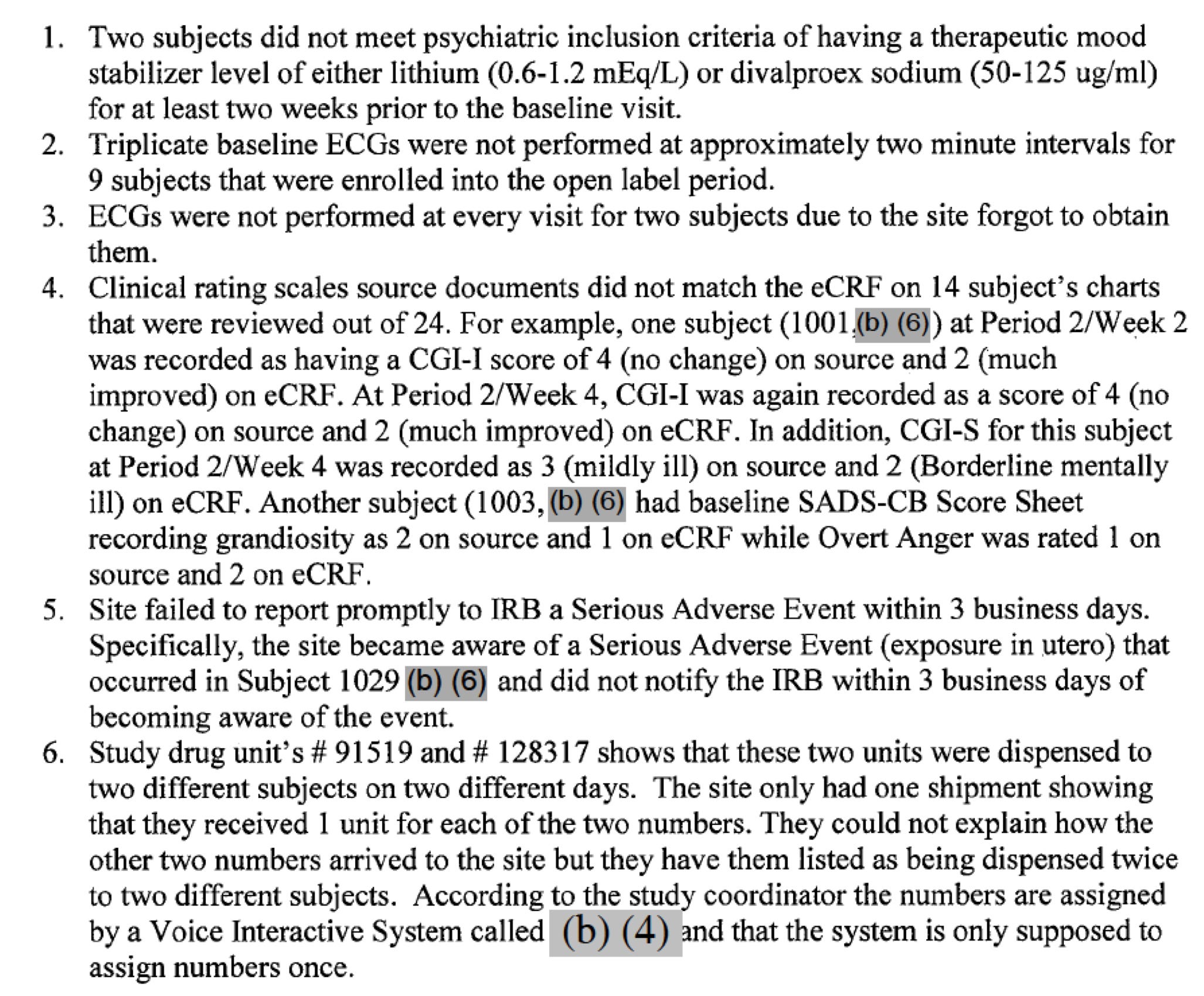
Those are the indicated conditions. Today, I learned that the entire back and forth between Pfizer and the FDA is available for this and all drugs! All study protocol violations are available. In the trial that gained approval for the use of Geodon as an augmentation agent in bipolar disorder patients who are already taking lithium or depakote (but, importantly, would later be prescribed alone or in combination with other non-studied agents), here is what happened at one particularly problematic study site:
The dirty little secret about antipsychotic medications? They aren’t THAT anti….psychotic. The whole class of dopamine-blocking antipsychotic medications have lesser standards by which they are judged for approval.
Most medications for psychiatric conditions have a “50% Reduction in Symptoms on Some Standard Rating Scale” compared to inactive placebo pills as a threshold.
“Is your intervention demonstrating efficacy in the “50% less miserable” range?”
This is the gold standard for good enoughness in depression medicine FDA approval trials. But… given the limited efficacy of antipsychotic medicines, the threshold was… adjusted for their approval.