


Defining Gender Affirming Care as “Child Abuse?" A Disaster.
The gripping tale of a series of unintended consequences from which Texas may never escape

We've had a “number of changes” in our world since I wrote this article. I decided it required revisiting, on the eve of new administration that's even more anti-trans than Texas alone.
I am a supporter of caring about trans and gender non-conforming youth. I'm a supporter of caring for children who need medical care, no matter who they are, and no matter what the problem. To be abundantly clear, as a physician who is a pediatric sub-specialist…none of us who work with these kids think abrupt decision-making is a good plan. No one who is a child psychiatrist is unfamiliar with the fact that children can and do change their minds. We're not excited about surgery, we're not excited about life changing drugs, unless that change is in the best possible direction. That direction is hard to know in advance. A stance that meets kids where they are, no matter what their problem, and tries to understand where they are in a developmental context is the best way to be a doctor for kids. It means working collaboratively with families, it means understanding different perspectives, and it means tolerating ambiguity. All of that becomes harder when gender variant kids feel under attack, which is absolutely what's happening culturally. I wrote this article at the beginning of the tidal wave of highly coordinated political advocacy for political gain. It used withholding healthcare for children as a football to win political points.
I'd like to get “the politics” out of the medical care. I think there are good reasons from a regulatory standpoint to do that. I think there are even better reasons for an ethical standpoint to get right with God about the fact that some kids are not gender conforming, and we have to have a rational and compassionate way to address that. We all need that. Every single one of us. Because even if you hate trans people generally, you probably don't hate people in your own family who turn out to have that sort of experience, and that's just going to be some fraction of the population. Maybe you'd rather have your kid have a bad outcome, but I doubt it.
This article is also written about two years ago, and I was a different writer than I am today. I'm avoiding editing it too much, a time capsule. I'd make different arguments and I'd probably write in a less… tortured manner today. But it's funny, it's got a lot of footnotes that are good, and I'm curious what my audience today thinks about what I wrote two years ago.
The point remain the same: compassionate and curious care about gender non-confirming youth is a good idea, and to do otherwise is a catastrophe when it comes to civil litigation. It's also a catastrophe when it comes to the lives of those kids, which is more important to me.
Don’t Mess With Texas.
If there’s one thing this column’s eponymous narrator, O. Scott Muir, M.D. loves, it is gonzo healthcare journalism and schadenfreude finding common cause. This regulatory Rube-Goldberg Machine is too much of an unbelievable 💩 show to pass up.
Now is the Winter of the Honorable Greg Abbott‘s Discontent
I’ve previously schaden-tweeted1 @2 the current Governor of Texas. According to an unattributed source on his official state website:
Named “Best Governor in the Nation” in 2020, Governor Gregory Abbott continues to build on his record as a strong conservative leader who fights to preserve Texas values.
But, spoiler alert, it’s not the National Governors Association that provided that particular “Best Governor” honorific!
I know. I’ll give us both a moment. It’s disappointing to me too. Breath…and…
It was the (deeply conservative) American Legislative Exchange Council (ALEC). It’s the kind of conflict-laden endorsement we’ve come to expect from “best male-performer Max Hardcore”, now being utilized by the GOP for their fans. A fan base, to be fair, with deadly anaphylactic reactions presumed to the memetic antigen that is “checking the facts.”
The Honorable Gregory Abbott has issued this executive decree:
Consistent with our correspondence in August 2021, the Office of the Attorney General (OAG) has now confirmed in the enclosed opinion that a number of so-called “sex change” procedures constitute child abuse under existing Texas law. Because the Texas Department of Family and Protective Services (DFPS) is responsible for protecting children from abuse, I hereby direct your agency to conduct a prompt and thorough investigation of any reported instances of these abusive procedures in the State of Texas.
As OAG Opinion No. KP-0401 makes clear, it is already against the law to subject Texas children to a wide variety of elective procedures for gender transitioning, including reassignment surgeries that can cause sterilization, mastectomies, removals of otherwise healthy body parts, and administration of puberty-blocking drugs or supraphysiologic doses of testosterone or estrogen3. See TEX. FAM. CODE § 261.001(1)(A)–(D) (defining “abuse”). Texas law imposes reporting requirements upon all licensed professionals who have direct contact with children who may be subject to such abuse, including doctors, nurses, and teachers, and provides criminal penalties for failure to report such child abuse. See id. §§ 261.101(b), 261.109(a-1). There are similar reporting requirements and criminal penalties for members of the general public. See id. §§ 261.101(a), 261.109(a).
Texas law also imposes a duty on DFPS to investigate the parents of a child who is subjected to these abusive gender-transitioning procedures, and on other state agencies to investigate licensed facilities where such procedures may occur. See TEX. FAM. CODE § 261.301(a)–(b). To protect Texas children from abuse, DFPS and all other state agencies must follow the law as explained in OAG.4
As astute readers of this column will note, I have italicized and bolded a portion of the above decree on the part Governor Abbott, which notes the reporting requirement for child abuse. Given the extremely broad definition of gender affirming care he has classified as child abuse, presumably because of his extensive experience as a pediatric plastic surgeon5, he also implicates every other licensed professional in the reporting of what he has now defined by executive order as criminal activity. Keep in mind, it would take two physicians to certify Govenor Abbott for involuntary commitment, with additional judicial review mandated within 72 hours. Only one of him—and at time scale of “at his whim”—is required to make the practice of standard-of-care medicine criminal.6
At this point, and this is a pro-tip to my friends at the ACLU7, please, please, please arrange a med mal lawsuit in which a general physician is found liable for a dereliction of duty resulting in direct damages8 in the care of a child after complying with this reporting mandate. It’s a contravention of the standards of professional ethics for doctors, so should not be a needle in a haystack to find those with legal standing.
Why would I advocate such a thing? Buckle up…
Medical Malpractice Carriers Don’t Cover Illegal Practice
Medical Malpractice insurance is conservative by nature and won’t cover things like non-hipaa compliant texting with patients or psilocybin assisted therapy cause, ya know, they’d lose.
Gonzo Journalism: It’s Not Just for Porn Awards Any More
In a recent phone call between two medical malpractice carriers and a child psychiatry colleague, the following opinion was obtained (twice):
[I] spoke with American Professional Agency underwriter and Allied World Insurance risk management with regards to how to approach cases of children with gender dysphoria here in Florida given anticipated legislation barring provision of standard of care treatments. They could offer me nothing concrete and could not confirm if they would continue to provide policies if such cases were successfully litigated in the state. If I can’t provide the standard of care and Something Happens to a kid because I was legally prevented to do so, I don’t see how I would win in that case. What are your thoughts?9
I called my medical malpractice carrier, and got predictably the same answer.

Of course it doesn’t end here, because refusing to see a patient because of the liability concern is, itself, something for which one could be found liable!10
All the Clouds That Have Lour’d Upon Our House: In the Deep Bosom of An ER Shift, Buried
Let’s imagine there is a child psychiatrist working for The Telehealth Company covering an emergency room shift. As the child psychiatrist on call, imagine a suicidal child is next in line Let’s imagine they have been evaluated for gender dysphoria. With around 41% of trans-identified individuals attempting suicide, this is highly likely. Let’s imagine the parents of that child took them to be evaluated for hormone-blocking treatment that morning for their gender dysphoria. Even if our Doc have no dog in the proverbial fight about gender affirming care in kids, she is still stuck. By virtue of her mandated reporter status, she is required to report both the parents and the pediatrician for the crime of child abuse:
Texas law requires that any person suspecting that a child has been abused or neglected must immediately make a report. If there is an emergency, call …
Professionals must make a report no later than the 48th hour after first suspecting a child has been abused or neglected or is a victim of an offense under Section 21.11, Penal Code. A professional may not delegate to or rely on another person to make the report (Texas Family Code, Section 261.101). …Professionals include teachers, nurses, doctors, day-care employees and others who are either licensed by the state or work in a facility licensed or operated by the state and who have direct contact with children in the course of their job (Texas Family Code, Section 261.101).
Or, within 48 hours, she is guilty of violating her duty to report.
Suspicion of “abuse” itself trips the mandatory reporting switch:
after first suspecting a child has been abused or neglected or is a victim of an offense under Section 21.11, Penal Code.
And inaction is further understood as a violation of one’s duty as a mandated reporter (from the DFPS legal guidance):
failure to make a reasonable effort to prevent an action by another person that results in physical injury that results in substantial harm to the child
Which has been redefined to include:
administration of puberty-blocking drugs
Or, of course, knowledge thereof. Sigh.
Through Me, You Enter the City of WoeBot
At this point, I’ll point out I’ve served as faculty at the Baylor College of Medicine in Houston, Texas. It’s pediatric teaching hospital is Texas Children’s Hospital. It had a Gender Affirming Medicine program. Which has of course been put on pause. Which is a defensive legal move. It also opens the clinic up to almost unfathomable medico-legal liability. According to national standards of care, to not provide the full array of appropriate options and needlessly report families is, itself, also defined as “child abuse” according to Texas DFPS:
—observable and material impairment in the child's growth, development, or psychological functioning;
—causing or permitting the child to be in a situation in which the child sustains a mental or emotional injury that results in an observable and material impairment in the child's growth, development, or psychological functioning;11
To push past objections regarding debatable harms, if we are speaking of suicide attempt or completion, I hope we can all agree that meets any possible definition of harm (e.g. “observable and material impairment”) No youth joyfully asks:
“Bruh, how was your suicide attempt last week?”
Much less receives the reassuring answer:
“kind of awesome, and completely absent any mental or emotional injury.”
This mandate has even opened the wormhole of legal horror that is the imminent collapse of the very Texas Department of Family Protective Services that is supposed to be the headsman for Governor Abbott’s politically popular execution (of his executive order—but it is a double entendre of which I am justly proud). Failure to investigate any allegations on the part of that agency itself is reportable…to the same agency…with the same dire consequences. This could lead to a möbius loop of iterative reports of failures to protect kids. It’s as if the serpent, in the garden of good and evil, had to file reports on its Apple Poising activities…with its own tail:
"For an agency already struggling, and often failing, to protect Texas children, the stakes are too high to ignore, according to the current and former employees, many of them supervisors and managers," wrote Chuck Lindell of the Statesman.
Actually abused children are almost certainly being actually harmed because the Honorable Governor is busy pursuing help-defined-as-harm. Political Action as new agency mission— over the objections of civil servants— is a poor employee retention plan in Child Protection circles, I would imagine. For them, such directives are anathema. You know, because they signed up for a job to protect children from harm.
The Anatomy of An Ethical Obligation
Physicians have ethical guidelines we have to follow by virtue of the privileges afforded by a medical license. Recall, these ethical codes and our adherence to them is why we are allowed to do things like “ask wildly invasive questions” and “cut people open” without going to jail for assault:
(From the American Psychiatric Association Code of Ethics, 2013)
Section 3
A physician shall respect the law and also recognize a responsibility to seek changes in those requirements which are contrary to the best interests of the patient.
It would seem self-evident that a psychiatrist who is a law-breaker might be ethically unsuited to practice his or her profession. When such illegal activities bear directly upon his or her practice, this would obviously be the case. However, in other instances, illegal activities such as those concerning the right to protest social injustices12 might not bear on either the image of the psychiatrist or the ability of the specific psychiatrist to treat his or her patient ethically and well. While no committee or board could offer prior assurance that any illegal activity would not be considered unethical, it is conceivable that an individual could violate a law without being guilty of professionally unethical behavior. Physicians lose no right of citizenship on entry into the profession of medicine.
In this case, is it conceivable that the only way to behave ethically might be to break the law?:
Section 8
A physician shall, while caring for a patient, regard responsibility to the patient as paramount.
1. Psychiatrists’ relationships with companies, organizations, the community, or larger society can affect their interactions with patients.
2. When the psychiatrist’s outside relationships conflict with the clinical needs of the patient, the psychiatrist must always consider the impact of such relationships and strive to resolve conflicts in a manner that the psychiatrist believes is likely to be beneficial to the patient.
It’s hard to argue that The Honorable governor Gregory Abbott is somehow the patient, so the Texas Children’s Hospital approach of not providing care because of the legal relationship a hospital has with his state government violates the ethical standard of patients coming first.
And it’s heavy handed, I’ll grant you, but these are extraordinary times:
Section 7
5. Psychiatrists shall not participate in torture.
In the above example, we can see that a psychiatrist who had no plan to manage a patient with gender dysphoria, in the process of evaluating patients in an emergency setting, still has a medical license that requires them to follow ethical guidelines.13 This physician is placed in the following impossible bind (forgive the recap, but this is complicated stuff and I want to make sure we got it):
—mandated to report what their professional society (AACAP in this case) considers an appropriate standard of care as child abuse. (Texas Section 21.11, Penal Code).
—this places The Honorable Governor Gregory Abbott’s legal dictate above a patient’s best interest (APA medical ethics section 8, subsection 2)
— being forced to refer a family for prosecution for child abuse for following standards-of-care for their child is participation in Torture. (APA medical ethics section 7, subsection 5)
My affirmative defense against accusations of sensationalism are as follows:
Definitions from Oxford Languages
tor·ture
/ˈtôrCHər/
noun
the action or practice of inflicting severe pain or suffering on someone as a punishment or in order to force them to do or say something.
Forcing children to continue suffering with gender dysphoria, and forbidding treatment or consideration thereof, which so often leads to the suicide is…torture.
Which is to say, it’s an action taken to inflict suffering to force someone to do something. Which is the express purpose of the gubernatorial decree, is it not?
If it was not so bad, we would expect less killing of one’s-young-self associated. But what do I know?
[Tennessee Williams-esque stage directions: a messenger rushes in handing our author a rumpled note, and exits stage left. Our narrator reviews the missive]
It seems I have produced award winning podcast journalism on the topic as an Rudin Medical Ethics and Humanities Fellow on this topic before14 ...The time flies, doesn’t it?
Our theoretical doctor above ethically can’t make that report, and legally can’t not make the report. And if she follows the law she is committing a dereliction of duty to follow a standard-of-care for the patient. She can’t even pass on evaluating the kiddo in this emergency setting without committing… medical malpractice. If sued, she can and should lose.
Subsequently her insurance would have to pay out on the claim. Medical Malpractice risk management starts to get nervous right about now.
Death and Taxes and Pre-Tax Health Benefits, Now Placed in Deadly Hate, One Against the Other
For historical reasons— Which, in the height of irony, first began in Houston Texas at a hospital overseen by the Baylor College of Medicine— employers paying for health insurance is tax exempt. You can pay people in money, or you can pay them in benefits, and when you pay them in benefits you don’t have to pay taxes. In order to make this legal according to the IRS, those benefits have to comply with regulations from a series of laws:
First, meet ERISA (The Employee Retirement and Security Act of 1974). The crucial thing to understand about this law is that it’s both employment law and tax law in one:
It sets minimum standards for most voluntarily established retirement and health plans in private industry to provide protection for individuals in these plans.
What minimum standards you ask? Great question! It turns out that as it applies to health plan, the most important rules for minimum standards in an ERISA covered health plan are the following, thanks to the Accountable Care Act (ACA):
The Affordable Care Act (ACA) requires …[plans] ensure a sufficient choice of providers and provide information to enrollees and prospective enrollees on the availability of in-network and out-of-network providers.
This is to say the coverage must be adequate. It can’t be theoretical coverage, it has to actually cover the care people might need. This, although obvious, turns out to be non-trivial. Federal oversight of adequacy returns in 2023. This includes quantitative measurements (thanks Kaiser Family Foundation!):
Time/distance standards – This type of standard is used to determine whether participating providers are geographically accessible
A.k.a it has to be close enough. Futher:
Minimum number of providers – Another standard establishes minimum provider-to-enrollee ratios.
There have to be a minimum number of providers for your problem. Now this minimum varies from locality to locality, but the minimum requirement is unlikely to be none whatsoever, which is the risk that we’re talking about in this case.
Also: The maximum wait time matters. That is another requirement. Behavioral health has its own specific limits here:
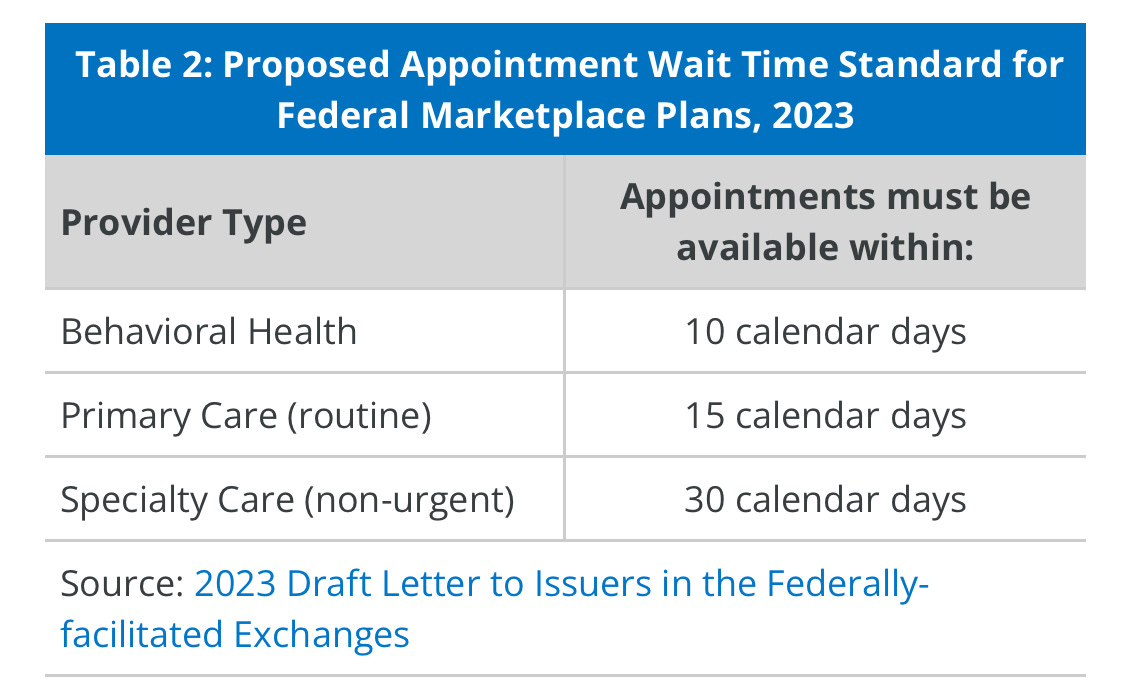
Imagine what happens to wait times when doctors start fleeing your state because they can’t get malpractice insurance thanks to your regulatory regime? Some deep weeds stuff also includes:
Essential community providers – In addition to other network standards, … [plans need to] contract with a minimum number of available essential community providers (ECP) in their service area. These include community health clinics, Ryan White providers, and other specified providers that serve predominately low-income and medically underserved individuals.
If anyone doesn’t think trans kids who are banned from care are medically underserved from the perspective of the IRS in forcing tax law, feel free to let me know. It almost doesn’t matter, because there’s so many other provisions that violates this is just kind of icing on the cake. And in 2022 the No Surprises Act added the following requirements:
The No Surprises Act requires all private health plans …to maintain accurate provider directories and requires providers to regularly update plans about any changes in their information. Plans must verify and update directories at least every 90 days and, on an ongoing basis, post any changes within 2 business days.
Suffice it to say that the reason that law was passed is not because all of the current provider directories are completely accurate and totally satisfactory. They are not. This is a big deal.
Welcome to the Force Function: Fiduciary Roles All Around
The term fiduciary has the following definition:
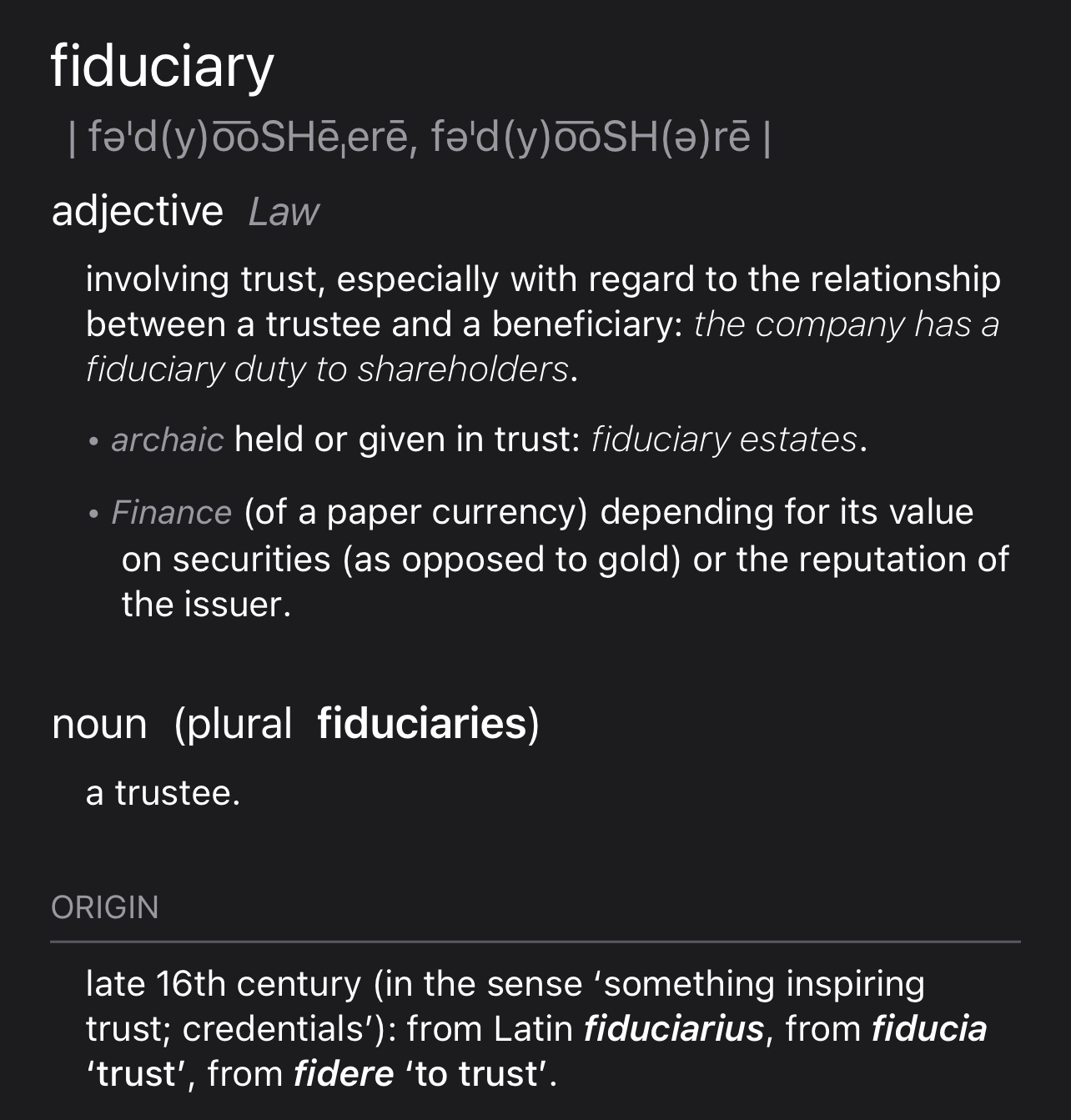
The ERISA law was initially a big deal because it required fiduciary duties for retirement plans. Retirement plans include money, and the requirement for plans to act as fiduciaries for their members made sense so they wouldn’t be ripped off with dubious investments that benefited only the person making the recommendation. The language around the fiduciary role of brokers and plan sponsors under ERISA that is now the law as of the combined appropriations act of 2021, and the language is basically copied from that same law as it applies to retirement plans.
As you can probably guess, the reason this needed to be put into the law is not because of the rampant freelance fiduciary duty assumption that was happening in the broker industry. It was, very much, the opposite. Brokers were for years allowed to take kickbacks. These kickbacks were paid by major payers like Blue Cross, united, etc. to sell their plans. And for some reason, we allowed this, brokers sold plans in their interest and not in the interest of plan members. That is now, to be very very very firm about it, not legal. However, unlike the relatively simple retirement plans—see what I did there? I refer to retirement plans as simple for effect—benefits are complicated.
Fiduciary Requirements: As we have seen above, the requirements have been laid out in a form that could be called clear. If you were a lying liar. More accurately, the standards would be called unbelievably complex to demonstrate despite the relative simplicity of the language and the clarity of intent. We can summarize what is necessary for a sufficient health plan under ERISA and it’s subsequent addenda (HITECH, MACRA, ACA, CA 2021, etc):
Time/distance standards
Minimum number of providers
Maximum wait time
Essential community providers
Up to date provider directory
Also, to be clear, It’s a big deal to violate ERISA:
The maximum criminal penalties for ERISA violations include up to 10 years in jail and fines of up to $100,000. Companies charged with ERISA violations can face criminal fines of up to $500,000, in addition to any civil liability.
This is why we can’t have nice things
To return full circle, I pointed out that actions like those taken by The Honorable Gregory Abbott of Texas create a paradox. They make the standard of care illegal, and pretty quickly, the sequela of that — medical malpractice lawsuits, doctors fleeing your state, etc— create what some of us in healthcare advocacy would consider an opportunity:
They create ERISA plan insufficiencies that are clear and unambiguous. This opens the door for definitive enforcement of the fiduciary rule under the CA 2020 law. Historically, ERISA insufficiency has been hard to litigate because plans could do a song and dance about how they really did have sufficient services, and it was a lot of work to prove they didn’t. But I’m going to prove to you, right now, with one example, how unbelievably easy it would be to make a claim against a Texas employer purchasing a theoretically ERISA compliant plan in the state of Texas:
What is the wait time for gender affirming care that includes “puberty blockers” in the state of Texas?
Answer: right now, infinite.
Standard violated: greater than 30 day minimum wait time.
What is the distance that any given patient or family has to travel within the state of Texas for gender affirming care that includes “puberty blockers” for youth?
Answer: the distance from wherever they happen to be in Texas to the nearest clinic in another state where they won’t go to jail for child abuse. And they still might if they come back to Texas afterwards.
Standard violated: maximum distance standards
What is the number of providers available to provide gender affirming care to trans youth in the state of Texas?
Answer: zero. All of them will go to jail if they do so.
Standard violated: minimum number of provider standards
State laws don’t change standards of medical care. They don’t change federal tax law. They don’t change federal employment law. No matter how much The Honorable Gregory Abbott would like to make Texas a sanctuary for those who deeply prefer no gender affirming anything, removing a medical subspecialty, and it’s associated care providers from the care available in a giant state like Texas causes every Texas employer – plan sponsors, most — and every Texas insurance plan selling ERISA compliant insurance A Serious Problem.
Texas: I Left My Heart In You
So here’s my moment of real schadenfreude cum triumph: I’ve been waiting for the ability to have a ERISA attorney file lawsuits that are just going to totally crush noncompliant plans. Why do I care? Cause it’s a breech of fiduciary duty and I have a personal vendetta against profiteering off of human suffering. I think the term might be morally injured?
This was gonna be really difficult. I was going to have to do all sorts of work to make sure we could document complex plan insufficiencies, it’s just really hard to do that. Unless the governor of a state does it for us. I hope the above amply demonstrated: Texas style anti-trans political opportunism makes health plans insufficient by definition.
I was going to end with some snarky line, but I’ll just use this photo from a recent rage against the machine concert instead:
Stop hurting kids. That’s…child abuse.
—O. Scott Muir, M.D.
Yes, this is a new word for schadenfreude in tweet format. For example:

It is a question of style that I consider unresolved as to whether tweeting at someone is best represented by the words “tweeting at“ or by using the “@“ as it’s actually used on Twitter to denote the action, and, given the underlying code, make the action manifest. In this case I am going to leave the stylist a question here in the footnote, and give the hipster use of the @ in the body text shot. Feel free to provide any sort of feedback on this “modern internet English” stylistic adaptation of otherwise traditional written English.
To make it very clear for readers, in youth, the standard of care is not to perform surgery. We understand as physicians that identity, including gender identity, is undergoing tremendous change in childhood and adolescence, and it would be in general a bad idea to start carving up children who might take issue with that plan later. So, the best interventions for pediatric gender dysphoria are social-emotional transition support, and reversible puberty blockers like Lupron. There are already extensive processes in place to obtain very thorough informed consent from everybody involved, thus the above prohibited medical procedures are already not standard of care, and that standard is constantly evolving and keeping with best available evidence.
Actually, I just checked, and he’s not a pediatric plastic surgeon at all! He’s not even any kind of pediatric sub specialist. It looks like he never even went to medical school? I am starting to get a little confused as to where his ability to practice medicine is coming coming from…oh. Wow. So he’s not a physician even in the Dr. Bill Frist sense… I wonder if this means Dr. Ben Carson is a mandator reporter about him also? The GOP needs to elect Mehmet Oz, M.D. with alacrity, it seems.
Medical certificates are crucial to the State in any commitment hearing. At the probable cause hearing, the State may prove its case based solely on the medical certificate if there is no objection. The criteria for medical certificates are set forth in §§574.009 and 574.011. A medical certificate is executed by a physician (not a psychologist) who has examined the patient within the previous 30 days.
For more on how much harder it is to commit someone to the hospital than it is to make sweeping rules about medical care, see: https://texaslawhelp.org/article/involuntary-commitment-texas
Yes, this is the very definition of medical malpractice
To prove I’m not making this up, private communication:
Which at this point could plausibly include living in the State of Texas.
Which one could argue is happening at this very moment in this very piece of writing, but to link to the top of the piece seems needlessly recursive. Let’s just imagine I’ve done that and move on, shall we?
Specifically, the guidance from the Texas medical board in this example case would be as follows:
If standard of care/treatment violations are at issue, all relevant information, including medical records, will be reviewed by at least two members of the TMB Expert Panel who are board-certified in the same or similar medical specialty as the respondent. If the resulting Expert Panel Report finds the respondent acted in a manner inconsistent with public health and welfare —including failure to meet the standard of care -- the case will be forwarded to the Litigation Section for further action.
The Rudin Medical Ethics and Humanities Fellowship is an extension of the medical humanities and biomedical ethics education that medical students and trainees receive at NYU Grossman School of Medicine and NYU Langone Health. A component of the Master Scholars Program in Humanistic Medicine, the fellowship supports learners with specialized research interests in the medical humanities and biomedical ethics. Yes, I’m a Fellow for work including:
Which, in full disclosure was actually recorded in San Antonio, Texas a number of years back with a graduate of Texas Tech medical school, which is located in Lubbock, Texas.