
"Bad Sleep:: -1"
It's a huge risk for suicide.

The Frontier Psychiatrists is proud to be just behind the vanguard1 of health-themed somewhat-satire publications 2023 featured an array of excellent articles, for a general audience, about drugs and their history.2. This year? I am taking a crack— in a reassuring format—for things that are not pharmaceuticals.
Today: Bad Sleep... Is it a valid clinical target worth resolving? In computer science speak, the title of this article is a joke…it refers to the Python search search for the liminal space that is the furthest away from the initial search term. In essence, the opposite, conceptually, of Bad Sleep in this case3.
“Most of us will spend approximately one-third of our lives asleep. Despite the large proportion of our existence that it consumes, there remains little scientific consensus regarding the actual function that sleep provides.”
Bad Sleep profoundly affects grumpiness and cognition.4
More Regular Sleep?: Effective Treatment Compared To More Sleep Alone for Being Tired and Sleepy
Starting with regular sleep, compared to just more sleep, we see that feeling tired and having daytime sleepiness is meaningfully addressed by having more regular sleep in a randomized control trial among otherwise healthy college students:
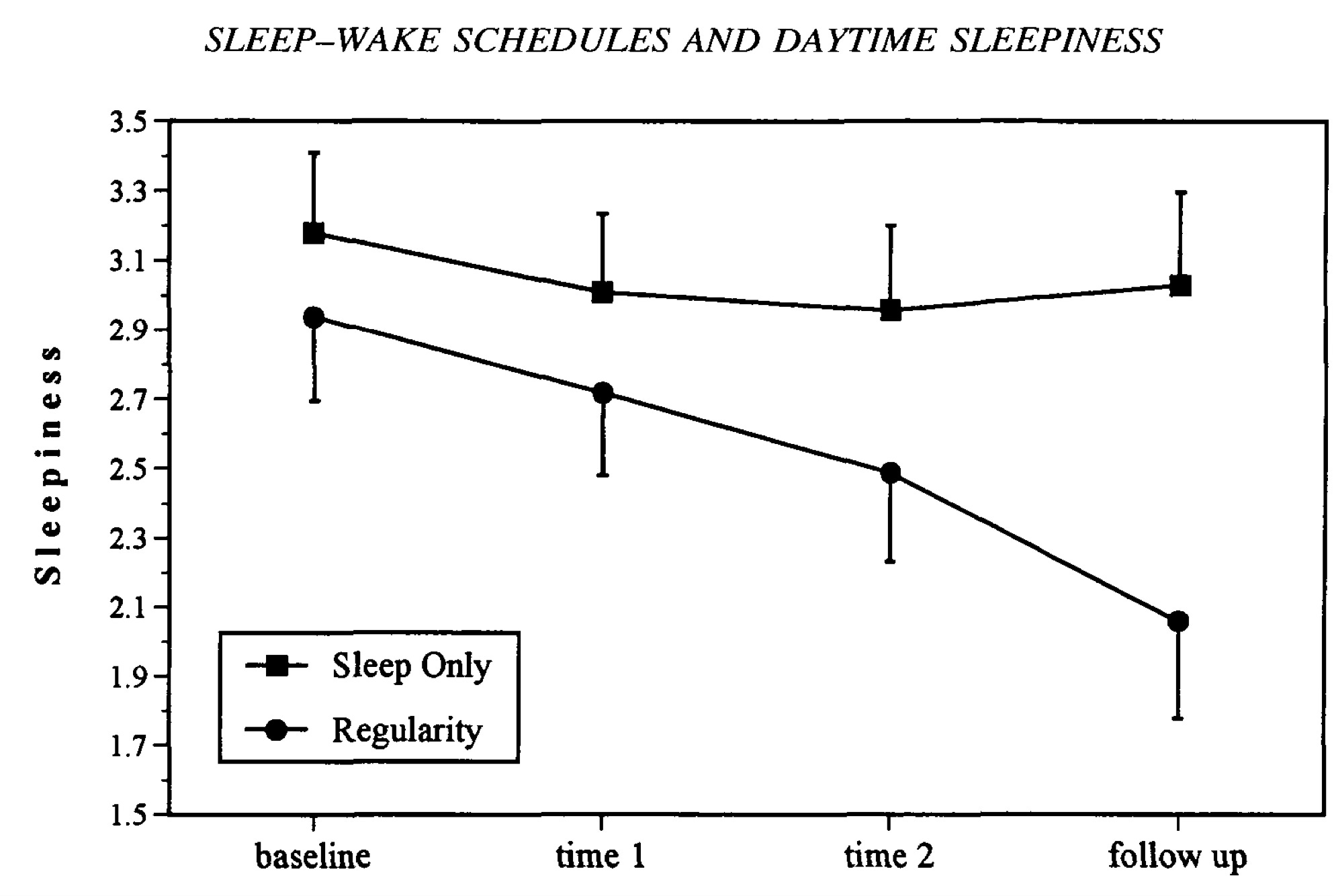
Subjects in the regularity group reported greater and longer-lasting improvements in daytime sleepiness. This improvement was observed despite the fact that during the 4 weeks of the experimental phase, subjects in the regularity group slept about half an hour less per 24-hour period compared to subjects in the sleep only group.5
Thus: good sleep is not just ENOUGH sleep, it’s regular and enough. Regular might matter more than just “enough.” Sorry, everything I wanted to believe in college.
Disrupted Sleep: It’s Bad for Adolescents
In adolescents, disrupted sleep is a serious matter—especially regarding risk for suicide— for those with co-occurring depression:
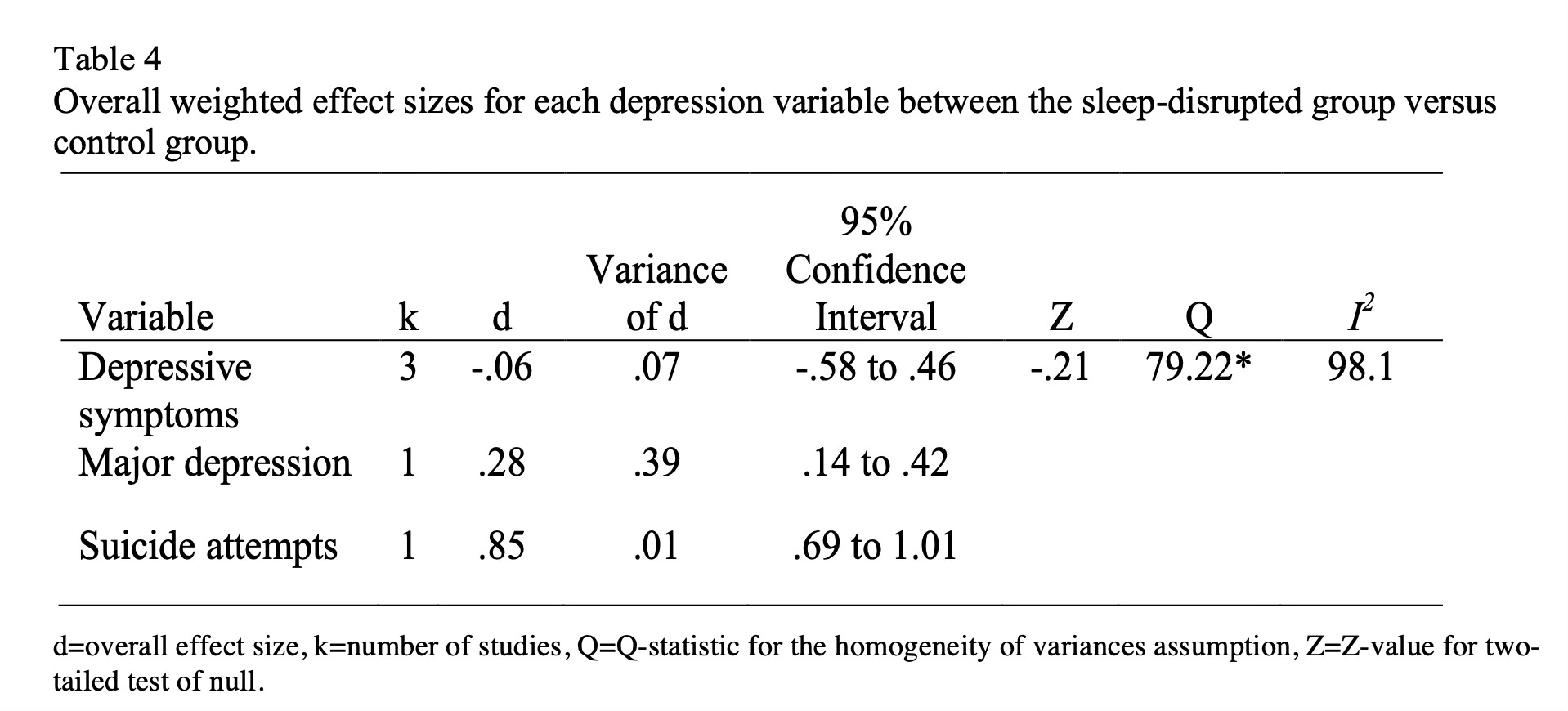
As we can see, the “Cohen’s d” (this is effect size—one of the Favorite Science Numbers for The Frontier Psychiatrists!) for the risk of major depression is elevated with high variance. Still, suicide attempts are VERY much more likely, and using the Muir-Skee Lo EQE (converting the 0.85 effect size into “inches of height lost” for this adverse interaction) equals a -2.125 inch height difference. It’s awful to have disrupted sleep when it comes to the risk of suicide attempts for adolescents.
Insomnia: It Can be An Independent Suicide Risk Factor
In an extensive cohort study (38,786 participants) from Sweden over a mean follow-up time of 19.2 years, researchers found that insomnia was an independent risk factor for death by suicide among people who got too little sleep (“short sleepers”):
The total effect of insomnia in the context of short sleep on suicide risk, expressed on the HR scale, was 2.85 (95% CI 1.42–5.74). The direct effect was 2.25 (95% CI 1.12–4.54) and the indirect effect, mediated by depression, was 1.27 (95% CI 1.05–1.53). Of the total effect, 32% was mediated by depression. The association between insomnia and suicide risk became more pronounced with decreasing depressive symptoms (p value for trend <0.05).
Suicide isn't all about depression; often, it's about impulse control, and impulse control is strongly mediated by sleep. There may be other factors involved as well, but it appears modifying insomnia is a potent way to prevent suicide among those at risk.
Nightmares and Insomnia: Significantly Associated With Suicide Risk
As reported by authors in the most niche journal that Owen Muir should probably subscribe to, “Suicidal Life Threat Behavior :6”
…nightmare duration [was] significantly associated with suicide risk independent of level of current nightmares, was tested using a linear regression. The overall regression was significant, N = 283, F(2,280) = 9.36, p < .01, R2 = .06, and both current level of nightmares, β = 0.18, p < .01, and nightmare duration, β = 0.16, p <.01, were significantly associated with suicide risk.
…as was associated with insomnia, again…
insomnia symptom duration [as] significantly associated with suicide risk independent of level of current insomnia symptoms … The overall regression was significant, N = 646, F(2,643) = 33.31, p < .01, R2 = .09, and … the level of insomnia symptoms, β = 0.23, p < .01, and insomnia symptom duration, β = 0.16, p <.01, were significantly associated with suicide risk. 7
The relationship between insomnia, nightmares, and suicide risk remained when controlling for everything other thing:
insomnia symptoms and nightmare duration were both associated with suicide risk after controlling for current depressive symptoms, anxiety symptoms, post traumatic symptoms, insomnia symptoms, and nightmares.
It’s an independent risk factor for completed suicide. The risk is huge in another cohort study8:
In a large prospective study, those who reported experiencing the occasional nightmare were 57% more likely to die by suicide, whereas those who reported experiencing frequent nightmares were 107% more likely to die by suicide.
Thank god we have novel therapeutics like the Nightware device that has an effect size of 0.88 for the treatment of nightmare disorder.9
It’s already an FDA breakthrough and will be discussed at Rapid Acting Mental Health Treatment 2024 this Sunday!
This is, of course, paid for by no commercial payers because why would we want to reduce the risk of completed suicide by half?
Bad Sleep: it can kill you.
Thus, I propose the opposite of bad sleep as a treatment. “Bad Sleep:: -1”…which means sleep should be:
enough
regular
at night
nightmare free
More than that is beyond the scope of this article, but it matters!
Outofpocket.health has vastly more subscribers and is also, according to Carlene MacMillan, MD , “pretty funny.”
This article is another in my series about one drug or another. Prior installments include Ambien, Prozac, Xanax, Klonopin, Lurasidone, Olanzapine, Zulranolone, Benzos, Caffeine, Semeglutide, Lamotrigine, Cocaine, Xylazine, Lithium, dextromethorphan/bupropion and Adderall, Gabapentin, and others.
Killgore, W. D. (2010). Effects of sleep deprivation on cognition. Progress in brain research, 185, 105-129.
Rachel Manber, Richard R. Bootzin, Christine Acebo, Mary A. Carskadon, The Effects of Regularizing Sleep-Wake Schedules on Daytime Sleepiness, Sleep, Volume 19, Issue 5, July 1996, Pages 432–441, https://doi.org/10.1093/sleep/19.5.432
As predicted by the journal title being right up the academic alley of the author Owen Muir based on the “he chose to mention it in the newsletter” scale of 1. That scale is rated 0 = not mentioned in the newsletter, to 1 = mentioned in the newsletter. This journal was rated a 1.
Nadorff, M. R., Nazem, S., & Fiske, A. (2013). Insomnia Symptoms, Nightmares and Suicide Risk: Duration of Sleep Disturbance Matters. Suicide & Life-Threatening Behavior, 43(2), 139. https://doi.org/10.1111/sltb.12003
Tanskanen A, Tuomilehto J, Viinamaki H, Vartiainen E, Lehtonen J, Puska P: Nightmares as predictors of suicide. Sleep 2001, 24:844-847.
Sleep is key
https://open.substack.com/pub/brain2mind/p/brainwashing-thats-good-for-your?r=wwc3t&utm_campaign=post&utm_medium=web
::weeps in ER doctor:: what’s...regular sleep?