

Focus on the Details: Committees in Medicine
Focus on the Details: Committees in Medicine
Carlene Macmillan, MD, and the role of committees and determining the healthcare for all of us
The Frontier Psychiatrists is a daily-enough health themed newsletter. Its editor—and writer for the majority—is Owen Scott Muir. Owen is married to Carlene. She is also a physician, and a much more serious person by a lot. Today, the day after Carlene was inducted as a Fellow of the Clinical TMS Society, I celebrate some of her accomplishments. She is the queen of details and the of the practical. I'm thrilled to re-introduce Carlene MacMillan, M.D., FCTMSS.

She does a LOT of committee work. For my general audience readership, in the world of medicine we have professionals societies, and they are “stacked” from subspecialty societies, then specialty societies, then the American Medical Association (AMA) when it comes to what codes exists to pay for which treatment. Those societies and sub societies are run by committees. These committees are similar to all groups of people—and we know how efficient groups of people are. There is a great reason startups have one or two cofounders, not 20. Nothing would get done. Unless, of course, you have amazing people who happen to be great at working with committees.
I’ll provide an example of when this matters. Let’s say we have a new treatment In psychiatry like SAINT neuromodulation. This is a now-commercial treatment that combines fMRI, an AI algorithm, and 10 TMS brain stimulation treatments a day.
There was a problem with this—there was no way to describe this treatment in the current billing and coding system. I have previously written about Current Procedural Terminology (“CPT Codes”)—a registered trademark of the AMA. This way of describing what medical care exists is owned by the AMA, and the government (specifically the center of Medicare and Medicaid services) by law has to use these codes. We could invent a cure for depression tomorrow—but no CPT code? No ability to get paid for providing it. It would take infinite years to get a cure for anything paid for if there was no CPT code to describe the procedure. Oral medicines have a different payment model, and IV drugs exist in both spheres at once. But procedures? They require a CPT code to happen.
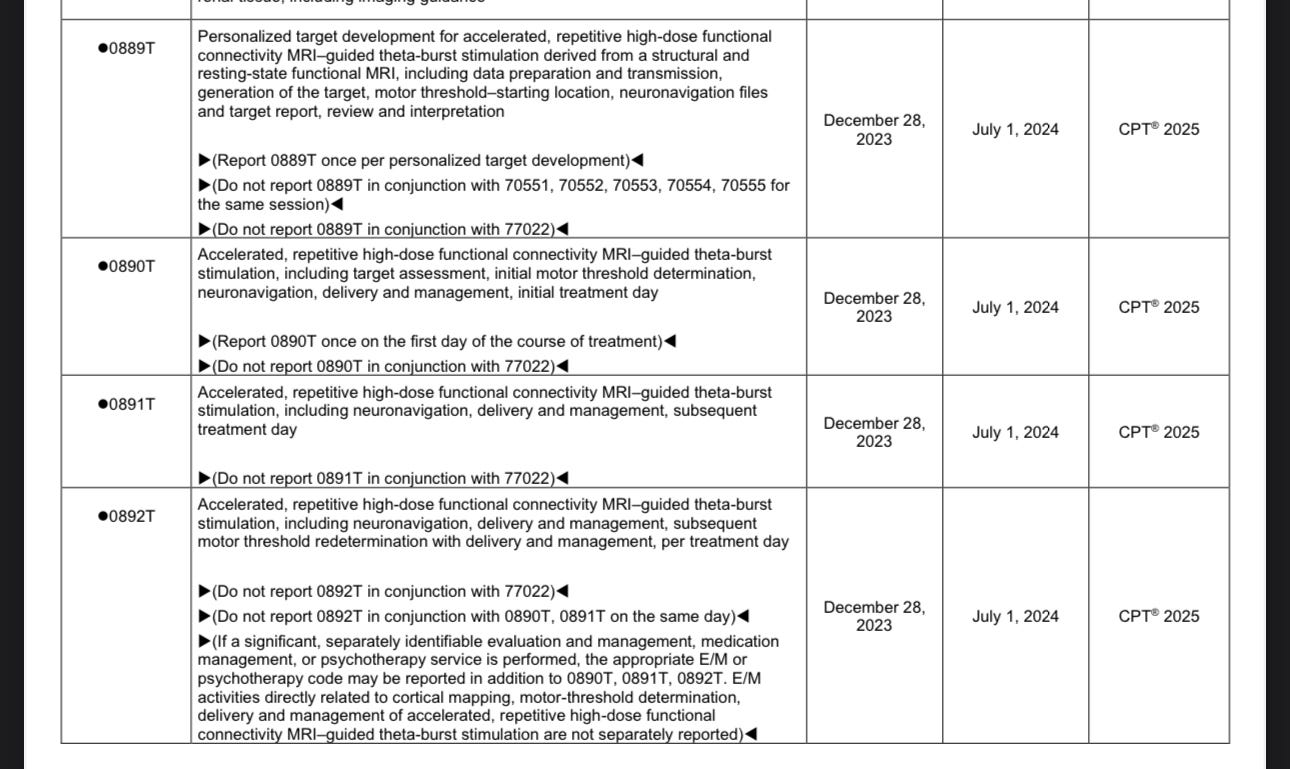
It’s a series of committees that need to consider these changes, and they all need to agree. To take the case of SAINT: new CPT codes were proposed. These needed to be supported by the subspecialty society—the Clinical TMS Society. That support needs to be communicated to the American Psychiatric Association—where Carlene has involved for over a decade. The professional society needs to support the new codes when they make their way to the AMA. The AMA has a consensus agenda for changes in CPT codes, and for items of dispute, they will debate them also. Others have unified consensus among the specialist societies advocating them. These items will be passed on a consent agenda on day one minute one of that meetings. So to get a new CPT code? Consensus all the way from most specialized to most broad. This doesn't happen on its own. Groups of people need to debate and come to a decision. Consensus decisions —at the end— are a lot easier to approve than issues of contentious debate. Building consensus is crucial if we're to have new treatments accessible to patients. It's a giant field of committees between an innovative new procedure and the ability to actually get that procedure paid for. Lo and behold: new CPT codes for neuronavigated fMRI guided Accelerated Transcranial Stimulation:
These might as well be landmines buried, blowing up the ability to get innovative treatments. I don't get to decide this is how it works, but it's definitely how it works. The most important committees in healthcare to decide on crucial topics like what is the multiplier for what a physician gets paid based on their “practice expense.” It cost more to run a surgical operation and then it does the traditional psychiatry office, the logic goes, and therefore we should pay surgeons more than Psychiatrists. This generally makes sense. It also precludes innovation that might require more overhead than initially imagined. A lack of consensus behind a treatment? We don't need to look a lot further than the dissenting comments raised during the FDA Advisory Committee for MDMA, who lacked expert consensus supporting the approval of the data, as submitted, for MDMA-AT. An advisory committee strongly weighing in against the approval by the subsequent FDA committee is likely to doom this FDA approval at this stage. Consensus of the experts makes things possible, and a lack of consensus blocks progress and bad ideas.
However, committees can change their mind. When presented with compelling data, committees can decide that a new thing should exist, or an old thing should be modified.
The ability to get depression to remission using accelerated treatment has a major barrier. That major barrier is called a medically unlikely edit, or MUE. It makes sense for CMS to not want to pay for more than one right knee surgery in the same day—it's considered medically unlikely that would happen. 100% of claims submitted for multiple right knee surgeries in one day? They will be bumped from payment systems. There is a piece of software, that's pushed out by the center for Medicare and Medicaid services, that build these in. Virtually every payer uses this software. For years, there has been a medically unlikely edit (MUE) that says that more than one TMS treatment in one day is medically unlikely. Thus will never get paid. Most providers didn't provide more than one TMS treatment in a day. Then they started to…
To be clear, I think accelerated TMS works better than once daily TMS. I think the data supports it, and I think it has for a long time.
Feel free to try out the Substack search function on this newsletter to explore the articles on the topic, or the science tab up to which links to my many publications on the topic in peer reviewed journals.
I have publication stating back to 2017 on the topic, and published hundreds of patients worth of data personally, and there are thousands published around the world. And still, until this year, the committee that decides on what is or is not paid for? Nobody asked if we could change the MUE on more than one TMS treatment in a day to allow more than one…no one even thought to ask. Carlene MacMillan did. With the backing of the insurance committee of CTMSS—of which she has been made, predictably, the co-chair— they requested a change to this highly medically likely sequence of procedures in the field. Stay tuned for the very end of the article to learn what happened—I wanted to re-create the experience of the committee for my readers ship, and these things take time, so you're gonna have to wait to find out if they were successful, also.
What about when the FDA announced clearance of TMS treatment for adolescent depression this spring? Families needed to be educated about the availability of this treatment. There's a committee for that too—the AACAP Consumer Issues Committee. Carlene MacMillan is also the co-chair of that committee. They created the following Facts For Families on this breakthrough treatment.

It's worth mentioning that although the committee members are unpaid, there are professional staffers, like that handsome gentleman in the lower right corner corner of the photograph, who happens to be named Rob Grant, who are employees of professional societies and to make all the gears turn in the background so that these committees have a place to meet, and have their decisions disseminated among other professionals. Staffers like Rob? Crucial.
Committee work? It is not paid. It is not glamorous. It's a lot of meetings in which cats are herded, motions are presented, seconded, debated, and consensus needs to be built. Consensus is built, motions might be passed, and those motions can turn into breakthrough treatments payment models, and a better world for us all.
Innovators who wave their hands are important. But at least in healthcare, they're powerless absent consensus support for their innovations. People with opinions, like myself, can't do much on our own. Even opinions plus data? Not treatments, until a committee reviews it. In medicine, real leaders? They build consensus. They do so in committees. Today, I celebrate the role of committees, and the people who serve on them. I will end this article with the sampling of committees on which Dr. Carlene Macmillan serves, at present:

APA: Member of Committee on Quality and Performance and member of Workgroup on Measurement-Based Care, Osmind Collaboration with PsychPRO Registry
AACAP: Consumer Issues Committee Co-Chair, AI Resource Group Member, and “Task Force to Review Operating Principles, Relationships with Industry, and Disclosure of Affiliations Process.”
ASKP3: Expert Faculty, Community Pillar co-lead
CTMSS: Board of Directors, Insurance Committee Co-chair
FACTMS: Board of Directors
New York County Psychiatric Society: Technology Committee Co-Chair
Thank you Dr. MacMillan, for moving the field forward.
Here's what's changed in the past year, thanks for the work many of the above committees: as of July 1, 2024, there are category three CPT codes that describe Stanford accelerated intelligent neural modulation treatment and fMRI guided accelerated treatments. So now the conversation can be had with a payer about what they would pay for that thing. One could never have that conversation successfully before the code existed. Industry played a role, but it's committees of medical professionals who decide what happens in the end. Additionally, without her, getting the medically unlikely edit for transcranial magnetic stimulation changed so that providers can do more than one treatment and have it be reimbursed in a day? That is changing, at least a little bit, too. The clinical TMS Society insurance committee submitted a letter to the center for Medicare to change to the MUE. That change was granted… A little bit. Starting July 1, 2024, up to two TMS treatments can be provided in one day. It's not 10, but it's not one. Change comes slowly in medicine.
This article was originally going to have an exciting ending, but I couldn't get it through ASENMS. That is, of course, the committee for the Advancement of Strong Endings in Niche Medical Substacks.
Three cheers for Carlene Macmillan, MD. Successfully pushing the rock up the hill for everybody!
Wow that's incredible. So Medicare will now cover 2x rTMS (non-neuronavigated) treatments a day? Is that national or subject to state adoption in local coverage determination? Private insurers will be playing catch up I'm assuming?