
What "Works" For Borderline Personality Disorder (BPD)?
Hint: it is not oral medicine or hospitals.

Borderline Personality Disorder (BPD) is a problematic name for a real Problem. A brief back-of-the-envelope description:
Imagine you had a Lamborghini as your first car. And you lived in a town with eternal snow and only steep hills. And everyone ripped on you for being a terrible driver while they rolled around in their AWD Subarus.
Now make the above about emotions. That is what it feels like to have BPD. It is maladaptive to drive in the snow with a car exquisitely tuned to do anything but that.
(My Book on A Therapy Mentioned!)
Although BPD is often present with other problems (Depression, ADHD, Etc) for which there are biological treatments, they are not treatments for BPD’s three core symptoms:
unstable interpersonal relationships
impulsivity
chronic feelings of emptiness
There are effective treatments for BPD, and they are all psychotherapeutic—not drugs or devices.
A recent meta analysis reviewed the state of pharmaceutical interventions:
Background: Borderline personality disorder (BPD) is a debilitating psychiatric disorder that affects 0.4-3.9% of the population in Western countries. Currently, no medications have been approved by regulatory agencies for the treatment of BPD. Nevertheless, up to 96% of patients with BPD receive at least one psychotropic medication.
And found the closest thing to a “f- no” you will see in a science article:
Out of 87 medications in use in clinical practice, we found studies on just nine. Overall, the evidence indicates that the efficacy of pharmacotherapies for the treatment of BPD is limited. Second-generation antipsychotics, anticonvulsants, and antidepressants were not able to consistently reduce the severity of BPD. Low-certainty evidence indicates that anticonvulsants can improve specific symptoms associated with BPD such as anger, aggression, and affective lability but the evidence is mostly limited to single studies. Second-generation antipsychotics had little effect on the severity of specific BPD symptoms, but they improved general psychiatric symptoms in patients with BPD.
Conclusions: Despite the common use of pharmacotherapies for patients with BPD, the available evidence does not support the efficacy of pharmacotherapies alone to reduce the severity of BPD.
Meds: Nope.
That leave us with therapy. As previously covered, The NY Times loves Dialectical Behavioral Therapy:
Louboutins are the Best Shoes We Have, Expert Says

I’ve got to give it to the New York Times: they know their audience. It is full of highly educated lefty white people with more than average income who like to protest things that they have strong opinions about. We also have a pathological need to be able to answer the question: “
New large-scale research supports others as well.
A large meta-analysis this year found that Therapy for BPD > Therapy Not For BPD:
We found a large effect size (g = 0.78, 95% CI: 0.56 to 1.01, p < 0.0001) favoring interventions for ‘borderline personality disorder’ (BPD) symptoms over Treatment as Usual or Waitlist (TAU/WL), and the efficacy was maintained at follow-up (g = 1.01, 95% CI: 0.37 to 1.65, p = 0.002).
This effect size converted to a height difference using the Muir-SkeeLo EQE = 2.5 inches taller!
Psychotherapy is hard to study in that you are limited to studying its effects on patients who can enroll in a research study—by definition, they are suffering enough to want “experimental therapy” but can hold their s@&$ together enough to make it to a bunch of study visits. That caveat aside, Therapy trials for BPD have done a better job than depression studies at enrolling generalizable patients, in my opinion. One issue is that the the research has been bedeviled by dropouts:
Schema therapy (ST) had the lowest dropout overall, and mentalization-based treatment (MBT) in the first two quarters. Community treatment by experts had the highest dropout. Moreover, individual therapy had lowest dropout, group therapy highest, with combined formats in-between. Other variables such as age or substance-use exclusion criteria were not associated with dropout.
Conclusion The findings do not support claims that all treatments are equal, and indicate that efforts to reduce dropout should focus on early stages of treatment and on group treatment.
In keeping with this newsletter's focus on treatment for suicidal individuals, we will focus there (comparing treatments for reducing Suicide) from JAMA Psychiatry:
We found that DBT, Mentalization Based Treatment (MBT) and ST (Schema Focused Therapy) were significantly more effective compared to Treatment As Usual (TAU) and (General Treatment) GT. These findings remained statistically significant after performing sensitivity analyses only including ‘full’ DBT-interventions, and therapies using combined formats (individual + group).
Beyond traditional therapy and pills, there is some emerging evidence on treatment with non invasive brain stimulation.
There is work I have published on Transcranial Magnetic Stimulation (TMS) in patients with and without Personality Disorders and Depression:
[dTMS] showed a reduction in depression scores in… patients with a comorbid personality disorder, p <.01, d=0.75.
Non-invasive brain stimulation helped symptoms of depression in BPD…
Conclusion: Results indicate that dTMS reduces depression symptoms in MDD patients with and without a comorbid personality disorder.
A newer review of non-invasive brain stimulation (aka TMS plus one study of tDCS) found promise:
According to impulsivity and emotional dysregulated domain improvements, NIBS in BPD appears to restore frontolimbic network deficiencies. NIBS seems also to modulate depressive features. Safety and tolerability profiles for each technique are discussed.
So What Do We Talk About?
Borderline Personality Disorder is treatable, and we have psychological (talk) therapies that specifically outperform treatment as usual. None of these are medication. We have hard to access brain stimulation…maybe. And we don't reimburse either of these easily; unlike medications. None of which “work.” These talk therapies? They are typically done in the outpatient setting, so they're not reimbursed like life-saving surgery.
Maybe they should be?
There is a fiction: therapy is for mild problems, medication is for severe problems. If you see a psychiatrist, it's because you need medication. If you see a therapist, it's because you don't need medication. The above formulation is almost entirely wrong.
Psychotherapy is a remarkably effective intervention for borderline personality disorder. This is a life-threatening condition for many. Thoughts or attempts to kill yourself is a symptom of the disorder. Although SAINT brain stimulation has promise in suicidal patients, therapy has robust evidence now.
I’ve coauthored one book published by Springer Nature on MBT therapy, but it costs money. Here is a free video version of the main ideas related to mentalization based treatment, one of the specialized options:
However, psychotherapy is considered outpatient mental health care, and it's poorly reimbursed. This is because the medical necessity criteria for outpatient mental health care assume people are, more or less, not trying end their life. To borrow from my favorite medical necessity guidelines over at Cigna:
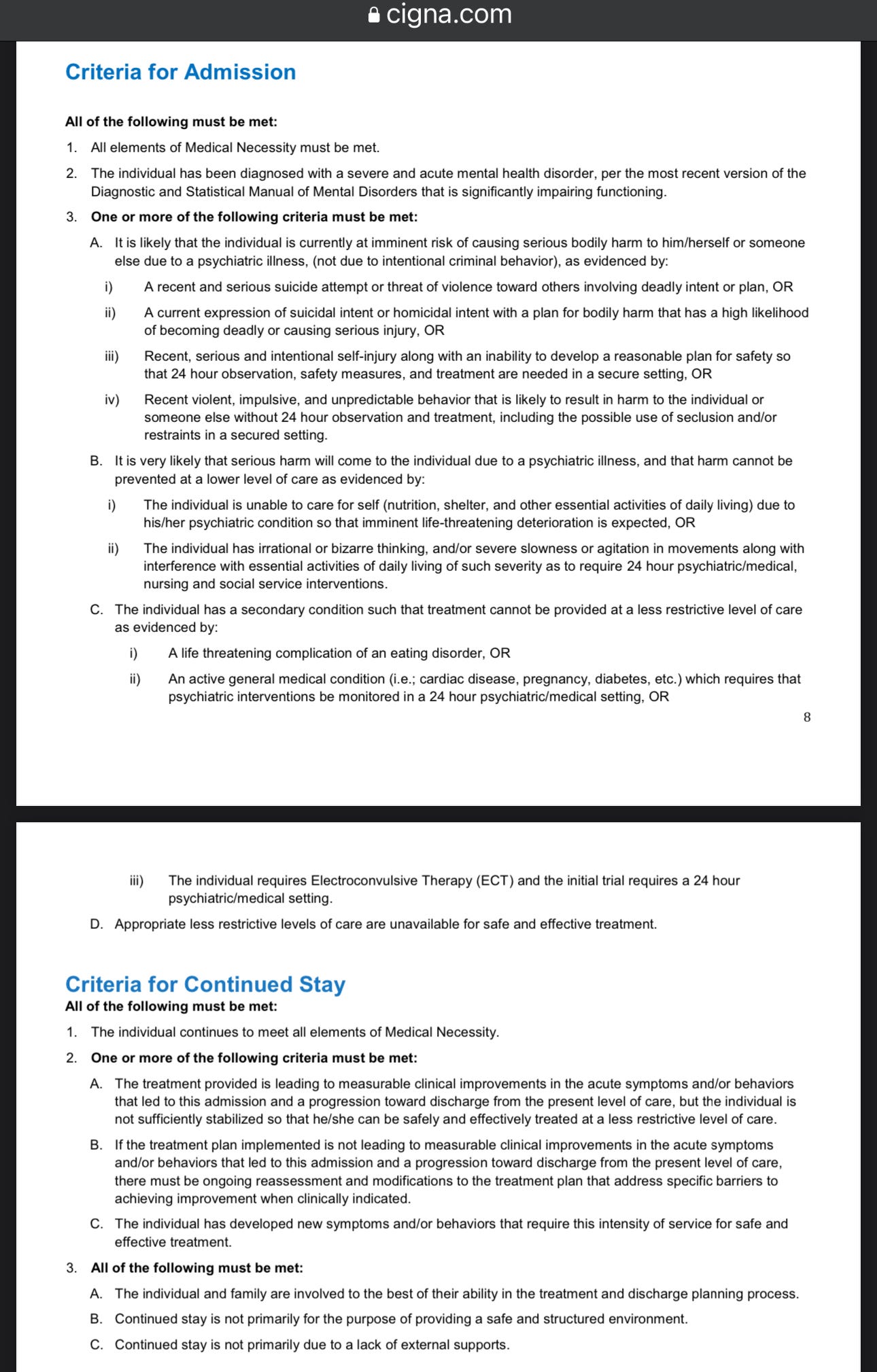
Given suicide attempts or ideation are among criteria for inpatient hospital level of medical necessity? Well, between that and outpatient care, it's tempting to imagine that our outpatients with BPD are not just not going to be attempting suicide—that care would not in keeping with what is medically necessary! This approach is the obvious and best way to mitigate risk. Define a risk as non-existent. This is unfortunately not factual for humans in their suffering. The facts matter less than the feelings. Just ask Romeo: (speaking to a sleeping Juliette but completing suicide anyway)
For fear of that I still will stay with thee
And never from this ⌜palace⌝ of dim night
Depart again. Here, here will I remain
With worms that are thy chambermaids. O, here
Will I set up my everlasting rest
And shake the yoke of inauspicious stars
From this world-wearied flesh! Eyes, look your last.
Arms, take your last embrace. And, lips, O, you
The doors of breath, seal with a righteous kiss
A dateless bargain to engrossing death.
We are left with the dilemma: what do you do about people who are suicidal but shouldn't be cared for in hospitals? If you define outpatient care as never including suicidal individuals, you exclude the possibility that very high risk suicidal individuals will be cared for in the outpatient setting. And you subsequently defined the payment models that support outpatient care … in a way that CANNOT including appropriate payment for high intensity or high acuity work outside the walls of the hospital.
Hospitals are not the best place to get your care for borderline personality disorder. Psychotherapy, performed by psychotherapy specialists, working with patients at risk for suicide, in the outpatient setting—that is what we have the data to support. It is happening in the real world. As a healthcare system, we pay for it like it's therapy for mild anxiety, not like lifesaving neurosurgical care for a “functional” brain problem that can otherwise kill you.
Psychotherapy and surgery can be similarly difficult, complex, and high intensity jobs. Some therapists do that complex work. Some surgeons do complex work, in emergency situations. Trauma surgery is a specialty. There is no emergency psychotherapy equivalent. I've been on a lot of plane rides in which the doctor on board was required. At least in my case, 100% of them had a psychiatric component to the emergency.
Our taxonomy has failed. Our payment models have failed. And it leaves patients with borderline personality disorder unable to get great care in the most appropriate settings. My emphatic suggestion:
Pay more for psychotherapists doing extremely difficult work. Train psychotherapists doing that work to a higher standard. Measure the work that they do relentlessly. Iterate.
We've seen this therapy-first model be scaled with NOCD when it comes to obsessive compulsive disorder treated with exposure and response prevention psychotherapy.
We cannot address completed suicide in the population by only talking about depression, “crisis,” and mutterings about “how important mental health” is. There are many drivers of suicidal behavior, and many drivers of completed suicide. One of those is borderline personality disorder, and it is best treated with expertise. Not drugs. And not hospitals, primarily. I discuss the in-hospital model here, from 2017:
A change? I don't want to be accused of being too impulsive given the subject matter, but the time is now. We have enough data. We have effective interventions. We need to scale our understanding of what therapy is capable of—it is not just dealing with minor problems, it is also for some of the most serious.
—Owen Scott Muir, M.D.
A fascinating read - I've read many of the usual resources about BPD and have dated someone in the past who was diagnosed and undergoing therapy, so I felt your starting analogy about a Lamborghini in the snow captured the dynamic brilliantly. I also agree with your general call to action, but I also suspect much of the general population needs engagement so people can understand and recognize their clinical options. I also wonder what aspect of the condition makes it so resistant to many treatment methods and modalities.