


The "First Line" Treatment Trap in Psychiatric Care
How brain stimulation treatment changes the lives of people with OCD...and its discontents.

I write about neuromodulation treatment frequently, and a criticism of existing data? The population studied is only treatment resistant patients. This article reviews OCD treatment with brain simulation via rTMS of various targets. I hope we will all learn something about science!
This is a newsletter by Owen Muir, M.D., and it’s worth subscribing to! This article is using an experimental new tool—included videos to explain stuff!
In the beginning, there were decisions made.
Like, for this article, defining terms!
Transcranial magnetic stimulation (TMS) involves taking an electromagnet and putting it close to your skull. When we repeat pulses, we put the “r” in front, to get rTMS.
Here is one picture that crushes explaining brain connectivity—how the brain syncs with itself in obsessive compulsive disorder:
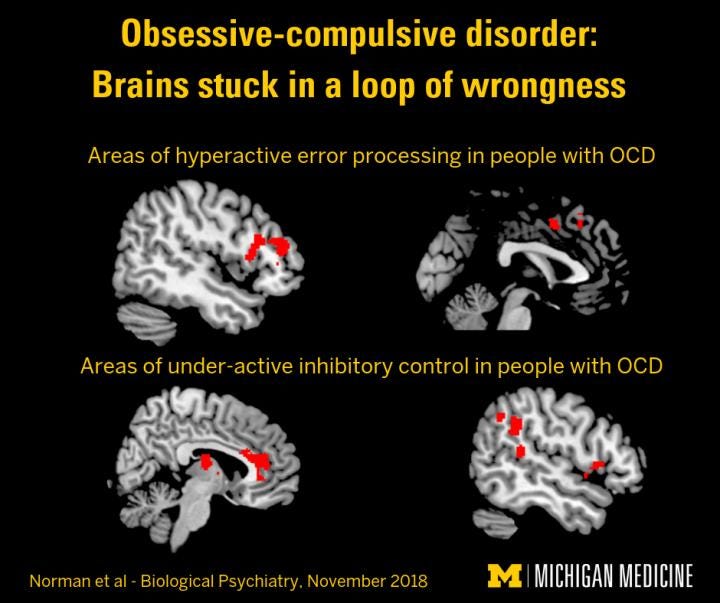
The OCD brain is stuck in a loop of wrongness.
I just love that explanation. Onward:
Mapping the Brain with TMS
Transcranial = from outside the skull to inside the skull. Cranium …