
Personality Disorders Exist
Yet are a poor excuse for executions

The Frontier Psychiatrists is a daily health-themed newsletter. It would be nice if I didn't have to write the following column. However, welcome to the world as we live today. I am not a supporter of physician-assisted suicide for psychiatric illness.
I'm going to start this column by using a screenshot of something that happened on the Internet today, in which somebody had the audacity (and perhaps grandiosity) to explain Paul McCartney's own song to …Sir Paul McCartney. It's like the narcissism that makes itself, but it's a great graphic to start this article with…were I to want to make the point that it’s possible to be so unaware of the perspectives of others that that they'd say the following:

Personality Disorders Exist!
There has been significant media coverage of the growth of physician-assisted suicide in the Netherlands, including its availability for young people with psychiatric illnesses. What follows is a public service announcement about the existence of illnesses that make people vulnerable to the terrible decision that is government-sponsored suicide. The first piece of news, for general audiences, is that not everybody has depression. There are illnesses, other than anxiety.
Some illnesses have to do with one’s sense of self, agency, and issues other than mood.
We accept that there are different types of cancers. Some kinds of cancer are very fatal, glioblastoma, pancreatic, cancer, etc. Cancer has different stages as well, stage one is different than stage four. Some cancers have a good prognosis, others have a very poor prognosis. There are differences. Psychiatric illnesses are a lot more cancer than we like to think.
Personality disorders have a name that's problematic for some. Still, if we can get past the name, I'm will describe what these problems are like, so we can, at least, accept, together, as an audience of readers, that these problems exist:
Individuals can have problems with, in one of a taxonomic system, four domains.
Identity
Self-direction
Empathy
Intimacy
Here is what severe and extreme problems in those domains look like, according to the alternate model for personality disorders in DSM-5:
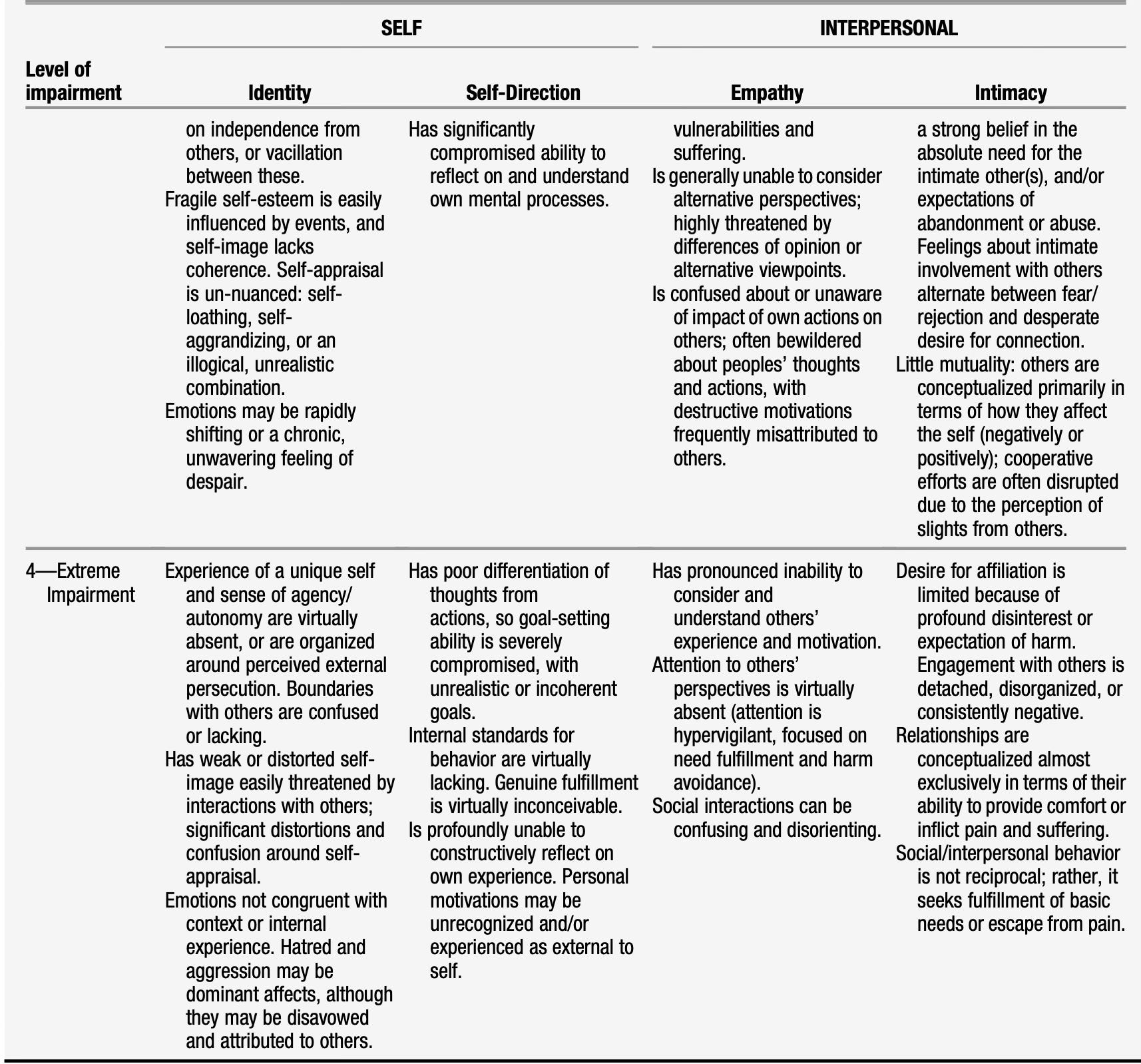
Now, with these anchor points handy, let’s take a look at the issue of physician-assisted suicide for “hopeless” psychiatric cases. This article hit the internet recently:
Since I am a psychiatrist, I can’t make a diagnosis of the person profiled. I can use this public profile of a person to ask general questions about what might be happening in cases of Borderline Personality Disorder, generally. Those questions will highlight personality disorder pathology such as having “emotions not congruent with context of internal experience” or “personal motivations may be unrecognized and/or experienced as external to the self,” as examples from the above table. Helpfully, the article includes some diagnostic information to work with:
“Ter Beek, who lives in a little Dutch town near the German border, once had ambitions to become a psychiatrist, but she was never able to muster the will to finish school or start a career. She said she was hobbled by her depression and autism and borderline personality disorder. Now she was tired of living—despite, she said, being in love with her boyfriend, a 40-year-old IT programmer, and living in a nice house with their two cats.
She recalled her psychiatrist telling her that they had tried everything, that “there’s nothing more we can do for you. It’s never gonna get any better.” [emphasis mine]
At that point, she said, she decided to die. “I was always very clear that if it doesn’t get better, I can’t do this anymore.” [emphasis, again, mine]
The first relevant point—the contention that individuals with BPD don’t get better, is altogether false almost all of the time. We know— this thanks to the diligent work of John Gunderson, M.D., Mary Zanarini, et. al. published in JAMA Psychiatry—the vast majority of patients with BPD get a heck of a lot better over time:
Ten-Year Course of Borderline Personality Disorder1
Results Eighty-five percent of patients with BPD remitted. Remission of BPD was slower than for MDD (P < .001) and minimally slower than for other personality disorders (P < .03). Twelve percent of patients with BPD relapsed, a rate less frequent and slower than for patients with MDD (P < .001) and other personality disorders (P = .008).
The actual answer? Well, in part, it’s just wait. It will get better. Subsequent publications from this same data set reveal the remission rate over 26 years is up to 99%.2. At least for BPD, the experience is overwhelmingly that things are hopeless. This may get less expert physicians to agree. The facts, however, are that improvement from BPD is as close to certain as we get with a medical condition. Keep in mind, in extremely impaired individuals, their sense of autonomy and a unique self is profoundly disturbed— or even absent. Thus, the suggestion, in these individuals, that death might be an “appropriate way out” is, itself, iatrogenic.
That's physician speak for the harm we cause patients. We shouldn't do that if we can avoid it, which in this case, we absolutely can.
The porous and suggestible sense of self and poor concept of agency is the problem…a problem that will, in almost everyone, improve with time. The following, if it doesn’t strike you as…off…well, that is an issue:
As if to advertise her hopelessness, ter Beek has a tattoo of a “tree of life” on her upper left arm, but “in reverse.”
This is undoubtedly her experience. It’s also common for patients with extreme impairment in personality functioning:
“Where the tree of life stands for growth and new beginnings,” she texted, “my tree is the opposite. It is losing its leaves, it is dying. And once the tree died, the bird flew out of it. I don’t see it as my soul leaving, but more as myself being freed from life.”
It’s almost as if attention to the perspectives of others, like her boyfriend, for example, is absent.
If we are going to offer physician-assisted suicide for patients with psychiatric illness, we need to understand the cohort who are going to be the most enthusiastic about it? They are those who will have a vastly higher likelihood of a personality disorder. Those individuals are also, paradoxically, most likely to go into remission later. Physician-assisted suicide for psychiatric disorders will inevitably— pointlessly—end the lives of individuals with personality disorders at disproportionate rates. This is a tragic and catastrophically misinformed decision. The argument that individuals with personality disorders are suffering because medication doesn't work is accurate: medication does not help those problems! It is almost completely beside the point.
It would be like providing physician-assisted suicide for arthritis— because antibiotics aren't helpful. That's not what antibiotics do. That's not what antibiotics are for. Arthritis requires nonsteroidal anti-inflammatories, or a knee replacement, or something—not vancomycin.
Similarly, although personality disorders are problems of the mind, they don't respond to traditional psychiatric medication, and instead require psychotherapy to get better—or, with all appropriate grim irony, just waiting it out for many people.
We shouldn't put people to death because they're impatient. We shouldn't offer death to children who can't wait for Christmas. We shouldn't offer death as an alternative to graduating high school. There are vast swaths of trials in this life that require waiting. Not being married yet— at age 16. Not having a job when you just lost one. Not having relief from your personality disorder at almost any age right now. Major depressive disorder can, of course, co-occur with these personality disorders, and still respond quite well to treatments like Stanford accelerated intelligent neuromodulation treatment, electroconvulsive therapy, and others. Other psychiatric conditions exist. I get it. They can suck. I have one. I know. It can feel really bad.
To say to young people, who have only tried traditional psychiatric medications, that we agree the future is hopeless? It's both false and needlessly punishing for people with a certain type of disorder— which the doctors ordering their death clearly don't understand.
We can’t have medical care be both so inept that it couldn't possibly help and, at the same time, be so certain of its abilities that we confidently consign our patients to the grave.
I don't doubt they're trying to relieve suffering, with the best intentions. I've seen those kinds of intentions before. They pave the road to hell.
Thanks for reading The Frontier Psychiatrists. Prior articles on borderline personality disorder and its treatment are below. Please consider subscribing, and becoming a paid subscriber.
There are over 558 articles in the back catalog for this newsletter, and they were a hell of a lot of work to create. I promise you'll get a lot out of them. But if you want to read them all, you have to become a paid subscriber.
Prior articles on Personality Disorders:
What is Borderline Personality Disorder?
Mentalization-Based Treatment for Personality Disorders III
Mentalization-Based Treatment for Personality Disorders II
Mentalization-Based Treatment for Personality Disorders I
Borderline Personality Disorder Book Club
And, of course…
Louboutins are the Best Shoes We Have, Expert Says

I’ve got to give it to the New York Times: they know their audience. It is full of highly educated lefty white people with more than average income who like to protest things that they have strong opinions about. We also have a pathological need to be able to answer the question: “
What Can Andrew Tate Teach Us About NPD?
What is OCPD and Do I Need to Worry About Explaining it Perfectly?
Gunderson, J. G., Stout, R. L., McGlashan, T. H., Shea, M. T., Morey, L. C., Grilo, C. M., ... & Skodol, A. E. (2011). Ten-year course of borderline personality disorder: psychopathology and function from the Collaborative Longitudinal Personality Disorders study. Archives of general psychiatry, 68(8), 827-837.
Temes, C. M., & Zanarini, M. C. (2018). The longitudinal course of borderline personality disorder. Psychiatric Clinics, 41(4), 685-694.
I had NO IDEA this sort of psychiatric "treatment" was going on. How wide-spread is this? What happened to "first do no harm."?
Nice article, thank you. When I first started in psychiatry in Scotland it was just about managing to avoid making patients with BPD worse (there was a long history of this). Now (or when I last practised), there had been what I perceived as a sea change in the approach clinicians took. I think it is amongst one of the most satisfying developments in therapy I witnessed during my career.