


Olanzapine
The frontier guide to psychiatric medications

This newsletter’s author is a psychiatrist, who is saying goodbye to “medication management” as part of his practice. As part of this decision, Owen is writing a series of articles summarizing what he learned about psychiatric medications as he makes the decision to see what happens when he focuses his efforts entirely on biological but non-once daily oral medication treatments. Neuromodulation is the future of the field…and in my day today practice, I focus on that new modality of neuromodulation
On the other hand, I spent years learning to manage oral medicines. So this article is about the trade offs in a sometimes life saving oral treatment.
A farewell to meds, as it were…
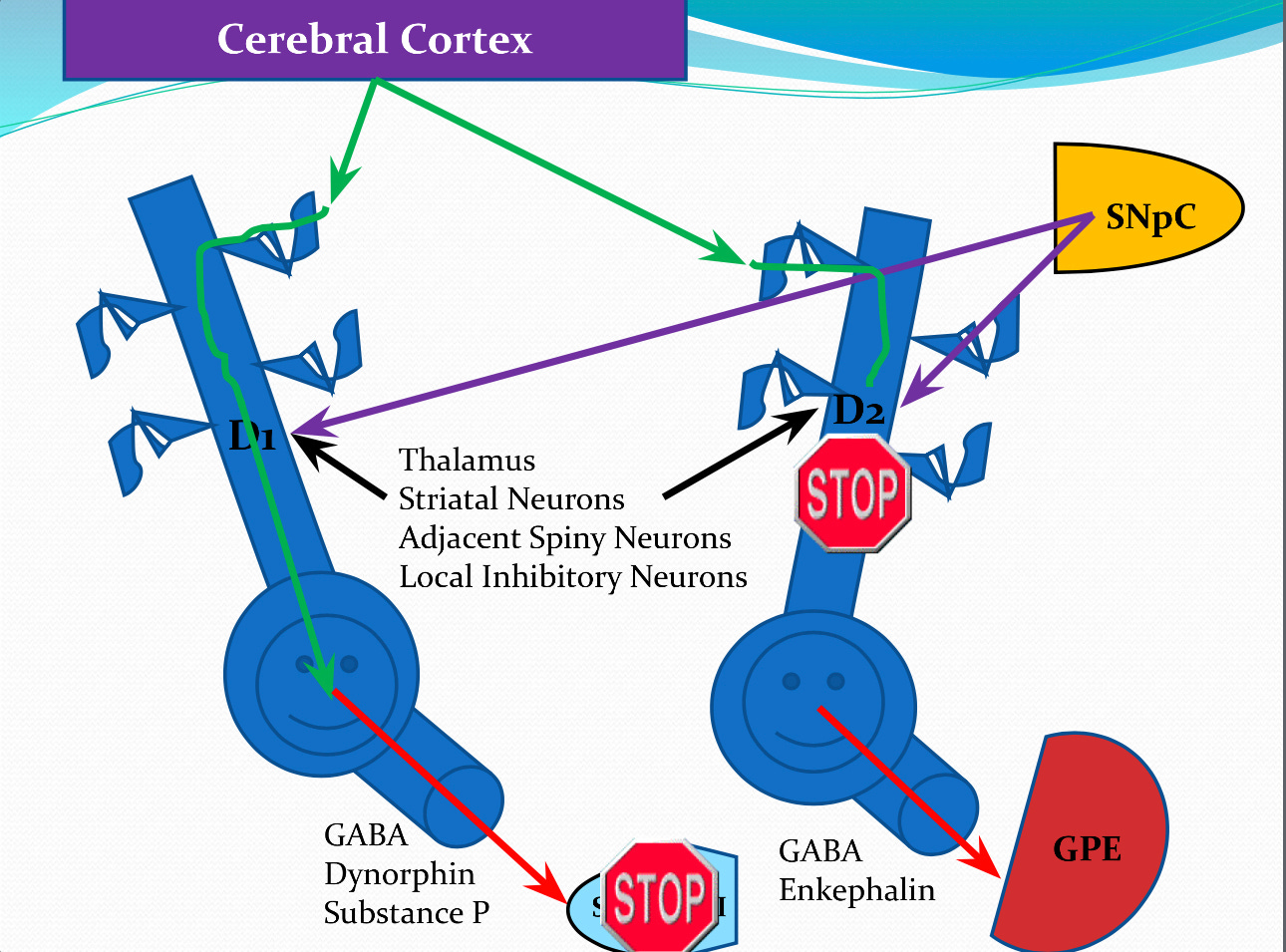
Olanzapine is the second “atypical antipsychotic” medication brought market after clozapine—Risperidone was the first. It was introduced in 1996. Antipsychotic medications are divided into before and after. An earlier generation of medications, starting with Thorazine, robustly blocked certain dopamine receptors in the brain— D2 receptors. The mechanistic role of D2 receptors has recently been called into question.
Dopamine. It's weird. It is the most popular of neurotransmitters in popular parlance. This is because of its role in the reward center of the brain, an area called the nucleus accumbens. Reward gets a lot of press. The crucial role of dopamine in the ventral striatum, attention, and movement is less flashy.
What is olanzapine (Zyprexa)?
Olanzapine is an atypical antipsychotic, and that means close to nothing. It blocks dopamine D2 receptors, and many other sites. As we've recently learned, this is far from the whole story when it comes to how these drugs act.
Our author believes that a lot of the receptor profile stuff that Psychiatrists obsess about is much ado about not much. I’m a brain circuit maxi, and only slightly interested in any individual receptor this or that. I think that's the way to sell the feeling of being an expert, brought to you by pharma.