
How Health Care Gets Paid for in America: Part II
Chapter 2: Levels of Medical Necessity.


Welcome to The Frontier Psychiatrists. It’s a Health-related newsletter and podcast, and poor-quality videos come out here, too. This is part II of my co-written FPs reader-requested exploration of the history and weirdness around healthcare payments…in the first installment, we met Pat, who fainted in a restaurant…and got IV fluids and a psychiatric evaluation in the ER. (this is a series…please go back and re-read that for context if you missed it). There is even a promotional message at the end.
Oops, I did it again...
When the emergency room psychiatrist arrives, Pat is exhausted and embarrassed by her day. She has a thought that many of us may have had in our darkest moments - “Is life even worth living anymore?” She immediately dismisses the thought - it WAS a beautiful day. She’ll remember to only go to restaurants during off hours. Manageable. She’ll wake up tomorrow, go to work, and not have lunch until 2 p.m. Easy Peasy.
There’s only one problem. Confused and with associated dehydration, she whispered her thoughts about life being not worth it out loud. She remembers that when she has lunch at her desk, she always remembers to take her medication - THAT’S what happened—she needs to take Geodon with food. She checks in with herself. She then looks up to see the psychiatrist filling out a form she recognizes. An admission form. Resigned, she agrees to be admitted to the acute care psychiatric setting.
How does this encounter translate into the world of medical billing and coding?
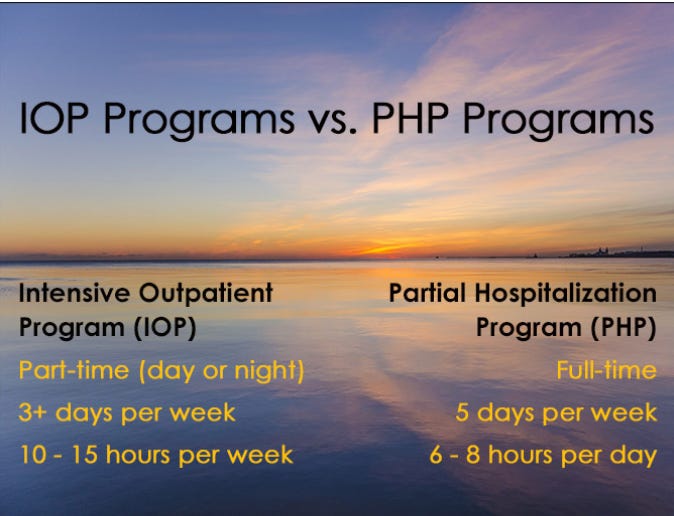
Pat ended up getting care in the ER. If you're getting care in the outpatient setting, you’re meeting a “level of medical necessity.” The medical necessity criteria for inpatient versus outpatient care in behavioral health have additional levels, including intensive outpatient programs (IOP) and partial hospitalization programs (PHP).
This generates different CPT codes and different billable amounts. Suppose you're doing the same care in an IOP versus a PHP versus an inpatient hospital versus an outpatient setting. It is presumed that the level of underlying illness you're dealing with as a doctor differs. I have written about this before, and it is a problem.
The “outpatient levels of medical necessity” include people who can collaboratively participate in their treatment plan. With a known history of high risk, inpatient care is medically necessary. Pat was sick enough to voice Suicidal Ideation in the ER. She probably needs to stay in a hospital - at least overnight, just to be monitored—this reduces the medico-legal liability for the doctor. In the past, when a worry-inducing medical event did not precede her thoughts of hurting herself, she’d been in a partial hospitalization program. Usually, she would progress to an intensive outpatient program. Eventually, once she could have a nice conversation and agree that their treatment plan was going great and she was feeling a lot better, she would graduate to outpatient visits in the clinic.
The criteria for determining the appropriate “level of care” for a patient in the outpatient setting are based on the patient's ability to actively participate in the treatment plan.
For the management of someone who's suicidal? The only place they exist, by definition, is in a hospital. If they're less suicidal than that, they're an IOP. Zero actively suicidal people are getting care in the outpatient setting according to medical necessity criteria. We understand that neurosurgeons see unwell, risky, and expensive to manage patients, not just in the OR. They also see them in the office. Their Relative Value Unit (RVU) math for their CPT codes includes this higher level of risk and expense as built into the RVU system that the basis for a negotiated payment rate based on:
time plus practice expense plus medical malpractice rates plus location
Neurological surgery physicians are always paid more per CPT code of any kind - because they are brain surgeons who get sued and have expensive operations.
Conversely, there is zero assumption that an outpatient psychiatrist ever sees an unwell patient requiring expensive or risky care—by definition, those exist and are paid for only in the context of higher levels of care—thus more risk and practice expense—in acute care hospitals, PHP, and IOP, never in the clinic.
Thus, care will not be well reimbursed for their expenditures unless you are a neurosurgeon working with psych patients. You never see sick people…because outpatients aren’t high-risk. Not because it’s true—but because it’s defined not to happen by the medical necessity criteria determining the amount reimbursed.
Physicians agreeing to care for Pat in the outpatient setting live in this strange nether world where they can write a bill with a relevant CPT code —90839 (psychotherapy for crisis). Still, since the setting is outpatient, it never pays enough because the medical necessity criteria say it’s only in the hospital setting that acutely suicidal patients exist, who would have the relevant practice expense and liability multipliers on the physician time spent. Outpatient mental health isn’t expensive enough according to the math behind CPT codes…and thus doesn’t generate the revenue needed to drive innovation with novel technologies.
The levels and levels of abstraction to get to a cost—instead of a value—are a problem. It creates an obfuscated center of gravity built on faulty anchoring heuristics. This leads to fewer resources to treat psychiatric illnesses and limited incentives for better outcomes. It creates so much confusion around the “why” that it’s hard to make change in a better direction—for patients— possible. It makes the shortest path to profits, ignoring risks and pursuing fast-cheap-out-of-control business models because the above mental math is boring and exhausting.
Thanks, readers, more to come! Good things come to those who make requests…and a special thank you to my friend, Sanjay, who helped co-write this piece. He's a baller.
Promotional message!
I have a webinar coming up with Al Lewis! Yes, that Al Lewis. (This is my legal disclosure of that affiliate link…to a book on “No One Believes The Numbers”). As part of your employer-sponsored health plan, we will discuss how your company can have next-generation psychiatric treatment—with the fancy BRAIN, SAINT, Monarch eTNS, and other treatments you read about here at a lower cost than you pay for care now—with a total of a 150,000 dollar value bet on that claim’s veracity. Sign up here for the Acacia Clinics x Validation Institute webinar!
 | A guest post by
|