

Ending Antidepressants III
Ending Antidepressants III
My conversation with Dr. Mark Horowitz from Outro Health continues.

Readers of The Frontier Psychiatrists, today’s article is part three of an interview with Dr. Mark Horowitz, MBBS, Ph.D. It has light editing. This is the third and final installment.
I’m your interviewer, Owen Scott Muir, M.D.
He’s a psychiatrist and co-founder of Outro Health. I’m an advisor to that company, too. They exist to allow patients to taper off of antidepressant medication safely. I’ve written about the lack of efficacy in these drugs before— Inessential Pharmacology. Mark’s book is the Maudsley Deprescribing Guide. It offers guidance to clinicians on how to safely discontinue these medicines.
In parts one and two, we learned that Mark trained as a psychiatrist and psychologist. However, his brain problems were offered treatment with medicines that, themselves, caused side effects, and those piled up to a disabling condition…and the thing that almost killed him…was trying to stop. The solution wasn’t what the doctors recommended…we then learned tapering off the medicines too fast almost killed him, an experience your author also had…
OM: I've been through a similar experience with pramipexole. As I wrote previously, it similarly almost killed me— Dopamine agonist withdrawal syndrome! I was following the taper my doctor prescribed. I went down from four milligrams, which is an insane dose, I later learned, down to 0.5 to 0.25mg. A month into the 0.25mg, I was thinking of pouring gasoline on myself:
The image of pouring gasoline over oneself and lighting a match is not a pleasant one. It’s not pleasant even when you’re thinking about someone else doing it, who is invariably a monk. Monks are in virtually all of the pictures that exist of this activity, because the most viewed image of this is on Rage of The Machine’s breakthrough album. Monks are different from regular people. Monks are not you or me on average. You don’t go to work wearing a monk outfits unless you’re a monk. Monks are conceptually far enough from early-40s, tubby, balding, white physicians as to allow for a sort of emotional and cognitive distance.
Your story, Mark, is very relatable. I also, it turns out, have something close to narcolepsy. Still, once you realize that you're chasing the dragon, as it were, with these medicines that you can't stop— is there the fear that, like traveling, going anywhere, is doing anything? “What if my supply of the medicine were to run out? Did you know that you were bound?
MH: Some of those thoughts did cross my mind. I think I'd had them before because I'd been on the drug for over ten years. I thought I'd always got to have the drug. I guess it became more clear to me. What I didn't realize? I was walking on a tight rope, three meters above the ground, and if I tripped, I would end up falling only three meters.
It did make me think about flying and having a supply of the drug. But I guess to me, the biggest dilemma was something slightly different, which was, as I was reading about people's experience on these drugs, I came across a lot of people who said exactly what I said. After starting these drugs, I fell asleep all the time during the day. I was diagnosed with narcolepsy.
And so I crystallized my thoughts, thinking maybe these drugs are what's causing my fatigue. I thought I was caught between a rock and a hard place here. I've been fatigued, which has caused incredible trouble in my life. It affected relationships and work. So, I had to accept this fatigue as I returned to those drugs that caused it. I thought being on this drug was causing me so much trouble in my life. It's hard to express the way it affects relationships. I miss events. I fall asleep. I arranged my life around naps; it's entirely consuming, and coming off this drug almost killed me.
Now, I'm back on a drug that's causing me all these health problems. Coming off, too, was incredibly dangerous. So, I felt trapped. I was! I'm trapped on a drug. It's causing me a lot of different, terrible side effects. And it looks like I can't come off it because it's too dangerous. So I felt I have no moves left on the chessboard.
OM: That's not the end of the story. Which is nice to know. Knowing the end of the story is always calming! People make a joke about playing 3D chess, and my response to that is that there are 10 ^ 40 moves available in chess. That's what's called the Shannon number. If you go to all the possible moves, including illegal moves in chess, you get 10123. On my math nerd soapbox, 3D chess requires more moves than there are atoms in the entire universe to calculate the change in those moves. There are between 1078 to 1082 atoms in the observable universe. That's not plausible. There are more than enough combinations on the regular chessboard. So here—running out of moves for being stuck on a drug— was a moment of…in the hero's journey, we’d call this “tests, allies, and enemies” or something like that?
You're also a psychiatrist and psychiatric researcher who has these tools at his disposal to do your job. What are you doing? That's what I'm thinking anyway.
MH: That's good. I appreciate you raising the stakes on this and making it more dramatic than it might be. So I'll tell you how I solved that issue. I was so shaken by what had happened coming off the drugs. I quit my job in London and moved back to my parent’s house in Sydney. I was an ostensibly grown adult human being in my thirties. But I ended up basically in a kind of crumpled mess on my parents’ floor. I, having moved out of the house ten years before, was so relieved when the symptoms went away after a few weeks back on a higher dose I put it to the back of my mind for a while.
I was back in Sydney, I was working as a psychiatry trainee, and I had this sort of thought in the back of my mind: these drugs are not quite what I had been taught they were. But I was just back in whatever role of life and trying to keep up with work, so it didn't occur to me—I was living relief.
Because I was back with my family, I had access to my parent’s private health insurance, which I didn't have in London. I ended up seeing more doctors. I was still quite confused. And I had doctors saying to me, you've got terrible narcolepsy. You need more different medications.
I still had terrible fatigue, and I wasn't confident at that point the drugs caused it. I had an inkling, but I wasn't certain. I followed their advice. I was given more drugs and more stimulants, which led to more anxiety, which led to more antidepressants. They tried these newer drugs, xyrem, and sleeping tablets. And I ended up on five drugs back in Sydney now a few years. And I didn't see it, but in retrospect, it's quite clear the more drugs I was on, the less able I was to function. I found work hard, memory, concentration. At some point, I decided to take a break from work. I went, and I took eight days of leave.
This is where it gets a little bit cliched. It turns into a kind of eat, pray, love. I went to do a yoga meditation retreat in Thailand. I couldn't be more of a bourgeoisie cliche if I tried. I did a lot of walking meditation there in a Thai jungle Buddhist temple.
And I thought, why am I on all these drugs? Have they improved my life? I decided I would try coming off them to see what's underneath. I solved that chess dilemma by following people who'd done it before me. So, it wasn't being trained as a psychiatrist. It wasn't psychiatric research. Recall there are 10^40 legal moves, but you said many more illegal moves in chess? I made one such move, not according to the rules I knew. I turned to peers on the internet.
They said you do it much more slowly than a few months, sometimes more than a year or even longer. You followed a specific pattern, reducing your most recent dose by 10 percent every month.
So it gets smaller and smaller. You can reduce by 10 milligrams at a hundred milligrams, but when you get down to 10 milligrams, you reduce by one milligram. There were all these people, actually tens of thousands of people, on these peer support sites saying when they followed this way of coming off antidepressants, it was easier.
It wasn't a walk in the park, but it was nothing like coming off over a few weeks, as most doctors recommend. I didn't have to work out anything myself. I had all these people saying, "This is what works." And the reason why I trusted them was that I tried the traditional way of coming off over a few weeks. I'd even gone slower. And it almost died. I knew who the experts were now. They weren't my professors at my university. There were these people online who, through trial and error, mother being the necessity, whatever necessity being the mother of invention being the mother of necessity, whatever it is, had worked out how to do it.
OM: The plural of anecdote is not data unless so many anecdotes exist?
MH: It depends on what you look at, what data is, and what anecdotes are. The data that my professors were basing their opinions on was that after eight weeks of exposure to antidepressants, most people have mild symptoms that last for a week or two.
OM: That's true. Most people can come off over four weeks.
MH: That's also true! Of course, at that point, I'd been on the drug for 13 years.
OM: So, they based it on the wrong sample.
MH: Exactly. It's a bit like crashing a car into a wall at 5km an hour and saying it's safe and extrapolating that to people driving around 80km an hour. In other words, the data that existed was not very good. In that context, looking at the hierarchy of evidence, 10,000 people talking about not being able to come off in one way and coming off in another way was the best data around. So, I followed what these people recommended on these websites.
And I thought, what's the harm? How can going off more slowly be wrong? I'm guessing the answer is that the experts were basing their opinions on the incorrect data. They had a very select data set of people who'd been on for brief periods.
OM: Why would pharma study people who were on for 13 years?
MH: They're just not in the available data. And the people online were a much larger group.
OM: They had a different biology.
MH: I think there are two important points to make here. First, drug companies are required to do 6—to 12-week studies to get their drugs approved by the FDA. That's why they do a 12-week study. And about, there's probably about a thousand studies of antidepressants done. 97 percent of them were done by drug companies. And 97 percent of them go for no more than 12 weeks. And there are no studies on long-term people who have stopped long-term antidepressants.
For example, the guidelines from the American Psychiatric Association today tell people how to stop antidepressants? They say you can stop over several weeks. And that is based on people who've been on the drugs for eight weeks. So, as you just said, the current evidence-based guidelines are only appropriate for short-term users.
Whereas in America, we know that half of people have used these drugs for five years or longer. And more and more people have been using them for ten years or longer. And we know that the longer you're on these drugs, the harder they are to stop.
OM: Yeah!
MH: Exactly—it's not that the people online have different biology; it's that they have been using drugs for a long time. Much longer than the studies. There are 46 million people on antidepressants in America. Twenty-three million of them have used it for more than five years. It's reaching 10 million plus, and I have been on it for over ten years.
OM: There's an insight that you recognize—which was that being on a drug for 10 years is not the same as being on a drug for 8 weeks.
MH: That's right. And data backs it up. Now, there's research that shows the longer you're on these drugs, the greater the chance of withdrawal effects and the greater the chance that they're severe. Which is obvious, of course, the longer you're on a drug, the more you adapt to it, the harder it is to stop it.
So, no, there's no rocket science there. What happened then to me was I took this approach. I took 10 percent a month approximately, and two major things happened. Number one, it was a lot easier to do that than to come off the medication more rapidly so I could tolerate the process. It wasn't horrible. Many of my symptoms also started to resolve as I came down off my drugs.
My tiredness improved, and my memory and concentration improved. That was the start of me realizing, very clearly, that it was these drugs doing it. That gave me a lot of hope and push to keep going. The second thing that I did was think this was utterly unbelievable.
I've got a PhD—in antidepressants!— from an institute that, while I was doing my PhD, passed Harvard as the most cited institute in the world. I'm trying to be a psychiatrist, but I'm getting more helpful advice from online peer support forums run by retired software engineers and homemakers. How is this happening?
So, I wrote an academic article combining the things I'd learned from this website with some academic research that reflected what was going on. I published that paper in Lancet Psychiatry. Over the last five years, that paper and the work around it have led to quite large changes in the guidelines in the UK [ed: NICE guidelines] on how to stop antidepressants.
It ended up being several papers. Number one was theoretical work, and number two was an observational study. So, the theoretical work is that we looked at the neuroimaging of antidepressants.
OM: Similar to Kapur’s work on antipsychotics?
MH: It's a Harvard guy, a guy called Jeffrey Mayer, who did in 2004; he scanned a whole lot of people on different doses of standard antidepressants. Look at how big the effect was on people's brains and what he found. Can I show you an image?
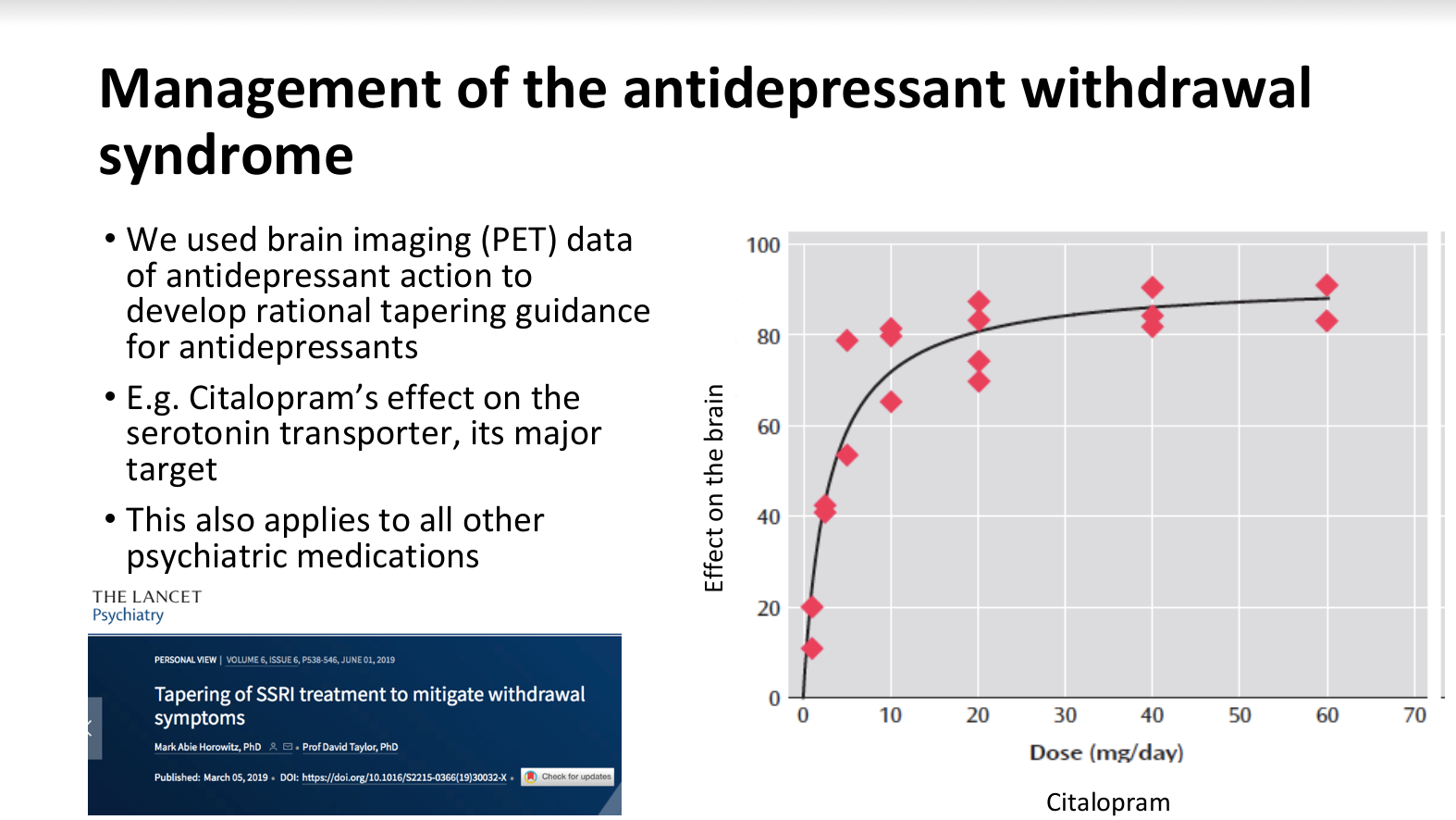
So, this is PET imaging of people on different doses of citalopram, a widespread medicine in America. It's looking at the drug's effect on the brain, which is inhibition of the serotonin transporter.
The key point is that the relationship between dose and effect is not a straight line. So, doubling from 20 milligrams to 40 milligrams doesn't double the effect on the brain. Huh. This is because of the law of mass action. When there's not much drug in the brain, all the receptors are unoccupied and “open for business.”
And so every milligram of drug has a significant effect, like the game of musical chairs at the beginning. It's very easy to find a chair by the time more and more of the drug is in the system; more and more receptors are occupied. So, every extra milligram of the drug has less and less effect. And that's why you get this sort of law of diminishing returns.
And so one of the consequences of this is very tiny doses of drug, like two milligrams, Which people would laugh at and say is a homeopathic dose has about half the effect of 20 or 60 milligrams. So tiny doses like 2 milligrams have much bigger effects than you would think. You can use this relationship to try to understand what happens when people follow the kind of advice that most doctors give.
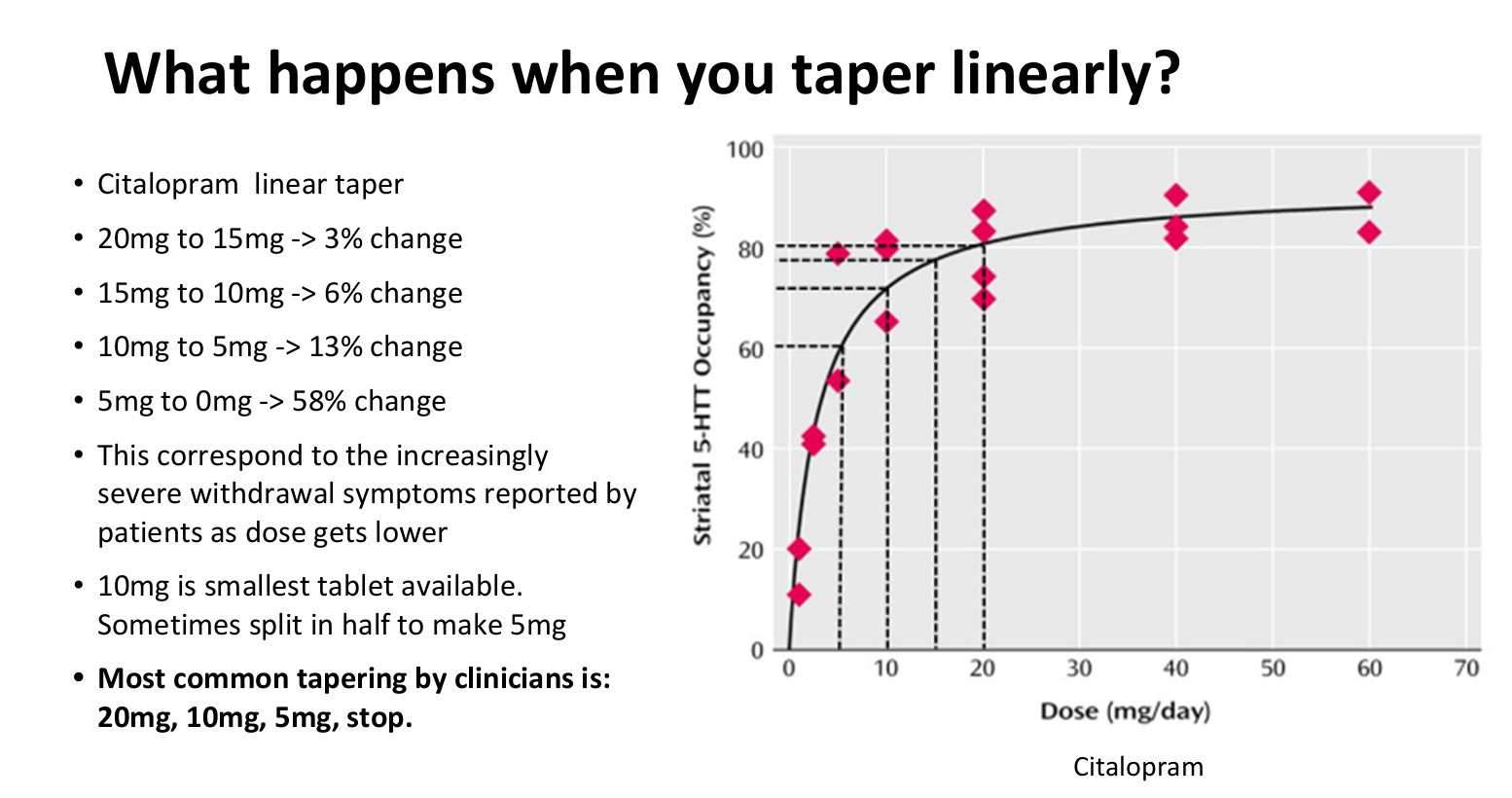
So, most doctors would recommend coming off 20 milligrams of citalopram by recommending halving the dose. And then half the dose again before stopping it is, but what your data shows is that no, essentially, stopping at five milligrams…
OM: you still have the vast majority of the effect of the drug to be rug-pulled…
MH: Exactly. You've got it. So you can imagine walking down. If this was a path, it starts as a garden path. You can walk very easily. It turns into a steep hill, and then it turns into a cliff.
OM: But there's a bias here because every doctor recommending to go down from 10 to 15 is correct. They get to feel better about their role as doctors again when someone goes from 15 to 10. And from 10 to 5, things go fine. So they have this smug sense that things are going to go fine.
MH: Yes, yes, exactly. People are a bit reassured because the earlier reductions are easy. This is going fine. Yes, my doctor has got things under control!
OM: But on both sides, it’s wrong! The doctors are convincing themselves they're doing a good job, and their patients are feeling like the doctors are doing the right thing. And there's no data to suggest to either party that it could be a disaster…until the cliff.
MH: Exactly. So what happens at the cliff is that people jump off. They can end up in a state of terror like I was. And because most doctors don't understand his relationship, they think they must need the drug; maybe the last five milligrams are the most important.
OM: Your depression has come back!
MH: Yes, exactly. So, they tend to misdiagnose relapse of depression or anxiety. I'm sure if I'd walked into any doctor's office, When I was panicked, terror stricken, I'm sure anyone would have said to me, you've relapsed clearly, your condition's gotten worse.
OM: I have a question for you: How long after a discontinuation or taper event can this kind of experience of horror and dread appear?
MH: It's a fascinating question because the textbooks say it should take three to five half-lives, which is about three to five days after most drugs.
OM: Those are textbooks about drugs. Not about neurons responding to what happens later, there's counter regulatory effects that the drugs have been doing for years.
MH: Perfect marks! Precisely. So, a study looked at the average onset of withdrawal effects in a cohort of patients. It found that it was about four weeks with a standard deviation of 13 weeks; in other words, it's enormous. It's a large variation, but what it's telling you is that some people experience withdrawal effects one, two, or three months after stopping their drugs. And there are two explanations for why that might be. Number one is “the mousetrap explanation,” which is that “you drop the ball. It hits the stick that presses the steps that do the whatever.”
OM: Rube Goldberg!
MH: It takes a while for things to unravel! Number two is based on a fascinating study that posits, “It takes a lot longer for the drugs to leave the central compartment than we think.”
For example, after a couple of weeks off a medicine, you can still see it affecting specific transporters inside the brain. In other words, the brain elimination half-life is longer than the plasma elimination half-life. Between those two explanations is probably why you can have withdrawal effects that come on weeks or even sometimes months after stopping the medicine.
OM: There isn't a “liver in the brain” to metabolize the drug. Most drug metabolism takes place in the liver for compounds in the blood, of course.
MH: Oh, you are asking if the drug must go into the blood across the blood-brain barrier and hit the liver? But there's another interesting study that shows that the elimination half-life in the brain is slower.
OM: And that fits with data from Kapur’s lab at UCL, where he showed with PET scan data that aripiprazole has this tremendously long half-life, and its dopamine receptor occupancy one week later is the same as on day one.
MH: That drug has a long half-life.
OM: But it also hangs out in the brain for a long time. And so does its active metabolite and blah, blah, blah, blah, blah. So, there are plenty of reasons why things could hang around longer. The drugs— if the unwinding of the effects is longer? It messes with the human ability to make a causal inference.
MH: You can imagine the doctors reading the textbooks. It says mild and brief symptoms come on two days afterward. Someone's in their office a month later.
OM: They look like death. They're sick. And it doesn't match the description in the textbook. So they think it can't be withdrawn.
MH: It must be terrible mental illness, relapse, something else. You can see where the trouble comes from! They are guided by short-term studies that underestimate the withdrawal effects, which cause havoc in clinical practice! Well, this means that doctors are reading books that are not accurate for their patients. That's huge trouble! We now have hundreds of thousands of people who have left their doctors and gone to online forums, just like me, because they find those forums more accurate and helpful than their doctors.
OM: Some people do have a mental illness—whatever that means and who are sick and could relapse.
MH: That exists. However, I want to problematize it a little bit. The vast majority of people who are prescribed antidepressants are prescribed by a GP or primary care physician; they've never seen a psychiatrist.
The vast majority of people who are prescribed antidepressants have mild to moderate conditions. The vast majority of people who have mild to moderate conditions see a GP or a primary care physician in the context of a major stressor: job loss, divorce, or physical illness.
OM: It's hard to have a relapse of a specific divorce.
MH: In other words, it's hard to have a relapse of a particular stressor in your life. Most people who are prescribed antidepressants do not have severe recurrent disorders. They have contextual stresses, which are in the past.
So, the idea of relapse, which is so prominent in doctors’ minds, isn’t often accurate, on average—the majority of starts on medicine are based on acute and non-recurring stressors.
OM: Essentially, this is my same argument about dubious “bipolar disorder.” If you treat everyone's “bipolar disorder” with Seroquel, it works for their “mania” 100 percent of the time—because they never had the underlying disorder.
MH: Yes. Doctors get to convince themselves they did a great job of preventing the relapse of mania in someone who doesn't have bipolar disorder.
OM: You argue that most people who are coming for help would be best served by someone helpful, listening, and supporting them psychosocially.
MH: I'm making two points. Number one, in most doctors' minds, relapse is the horse, and withdrawal is the zebra. I think the data is clear.
OM: The overwhelming majority of people have been prescribed these medicines for mild problems that are in their lives?
MH: That the horse is withdrawal and relapses is the zebra for most people, some people, there's some, there's people out there with very severe conditions, but that's not most people and do exactly what you're saying.
The NICE guidelines in the UK, which evaluate cost-effectiveness, found that the most cost-effective treatment for even severe depression was problem-solving therapy:
That means you tell somebody what your three major problems are. What's the first step to take for each one? And report back in two weeks on progress or barriers encountered. That's more effective, and that's more cost-effective than antidepressants. It's more even cost-effective than various forms of psychotherapies.
I think that gets to the heart of the issue: people. It's the things going on in their lives that tend to explain why people are miserable and anxious, and there are lots of ways to help them with that, of which I think only one is an antidepressant. And I believe that the way that antidepressants generally work is they numb people's emotions.
I don't know how much there are all these kinds of descriptions of biological effects and neurogenesis and inflammation that I was very Taken by, but I think when you ask most people on antidepressants, they say they feel emotionally restricted or numbed. And that's why people can feel better in the short term, which is a bit different from fixing their problems.
OM: It's fascinating that you've landed on the opposite end of the spectrum as I have in my career as a physician. I focus on very high-acuity individuals but have come to similar conclusions about the utility of these drugs.
In summary, if I am getting this right, in the world of primary care—where, on average, patients don't have a severe chronic psychiatric problem—these drugs are causing one. In the world of high acuity problems, where you do have a severe problem, the drugs aren't solving those. Riffing on what Dan Karlin once said to me, we perfected the algorithms to make these compounds as safe as water, at least initially. We have a generation of agents with the potency of water, but similar to withdrawal from water, that can be fatal, too.
Thanks for joining us for this three-part series!
My books (amazon links):
The Hellthread: Collected Poems
Why We Skeet: Further Collected Poems
Adolescent Suicide and Self-Injury: Mentalizing Theory and Treatment
Great series! I appreciate the PET data! I haven't had patients have issues with escitalopram discontinuation beyond a few days, but for SNRIs and paroxetine, quite a few have had difficulty.
I know someone on antidepressants for years and has dementia