



The path from xanomeline to the brand name treatment named Cobenfy was a long one. Cobenfy is FDA-approved for the treatment of Schizophrenia. Here is the literal label:
COBENFY is a combination of xanomeline, a muscarinic agonist, and trospium chloride, a muscarinic antagonist, indicated for the treatment of schizophrenia in adults.
To people who haven't yet read my book Inessential Pharmacology, (Amazon Affiliate Link), I will highlight that this is approved as a monotherapy. That means it can be prescribed as the only drug for people with Schizophrenia.
It has a completely different mechanism from every other antipsychotic. All the others block or modulate dopamine to some degree. Those are the variety of drugs I have written about, in less than glowing terms, in some cases.
These are medicines that lead to obesity and early death (particularly in youth on Medicaid). I have argued they should never be used as augmentation agents.
I argue, in fairness, a lot of things.
One of the things I have argued about regularly is that individuals, particularly those suffering from devastating illnesses like schizophrenia, deserve treatment that works. That same treatment best if it doesn't harm the person also. The problem with antipsychotic medication is that they regularly harm the people who take them.
Finally, we have a new drug that is helpful for individuals with schizophrenia and less harmful in terms of catastrophic adverse events like massive weight gain and tardive dyskinesia.
What are the adverse effects for Cobenfy? Yes, those used to be called side effects.
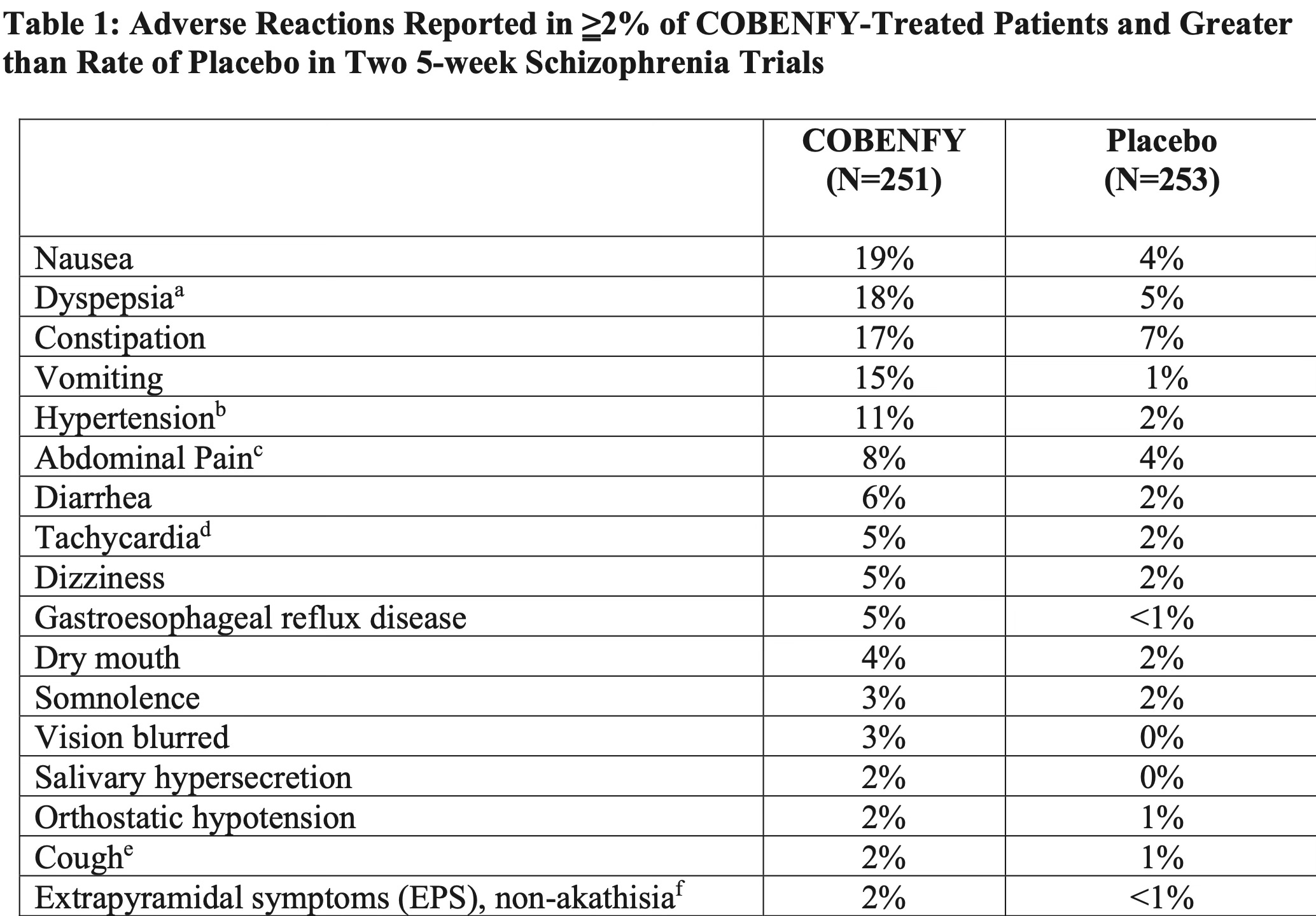
It's overwhelmingly causing problems related to nausea or other predictable anticholinergic side effects in the peripheral nervous system, especially the G.I. tract. I'm not saying it doesn't suck. I'm not saying it doesn't have side effects. But what you don't see there is massive weight gain. What you don't see there is permanent movement disorders.
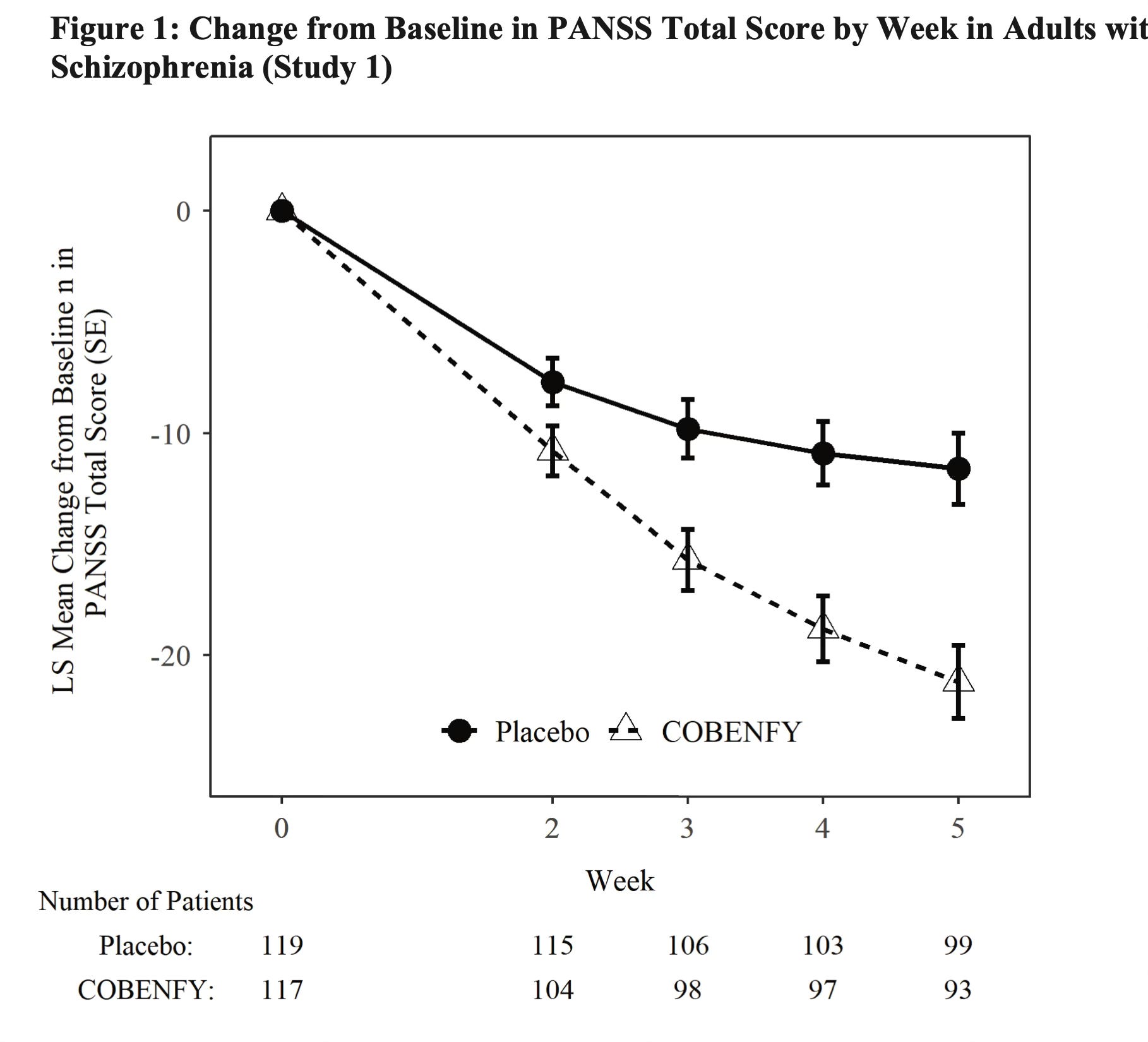
Does it work? In short, yes, it works. Nothing works fabulously well in schizophrenia yet, but it's not a slouch treatment, and it's not worse than existing drugs at least in the people they already studied (again, from their submission to the FDA):
It's the first not me-too for schizophrenia, since clozapine.
It's got a restricted range of side effects that are annoying, but not life-threatening. Will we discover more at large scale? Probably.
Bristol Meyers Squibb is not done yet. They are going to be bringing this drug to bipolar disorder, and other conditions. Let's reduce the risk of early death from dopamine blocking medications for everyone for whom that would be beneficial.
I'm at a conference, so I'll keep this one concise, because I'm writing it on my phone.
To be fair, TD doesn’t typically present until patients have been on at least 3 months of dopamine blocking medication and this study was only 5 weeks. Based on moa, the development of TD seems unlikely, but only time will tell. Postmarketing experiences should be enlightening.