
Are Oral Psychiatric Medicines Driving Obesity?
Evidence mounts, even without antipsychotic augmentation

The Frontier Psychiatrists is a daily health-themed newsletter. Regular readers have either enjoyed or felt grimly satisfied as I routinely address the adverse effects of psychiatric medications, usually focusing on antipsychotic and benzodiazepine medications. This is not to say these are bad medicines. These are occasionally life-saving medicines. It generally emphasizes the need to balance risks and benefits, And that means acknowledging risks.
We all know obesity is a problem. Many have been content to gloss over the problem of medication-induced weight gain—until it became a real economic problem. The remarkable success of GLP-1 inhibitors in the market, as well as ever-increasing data about their effectiveness and weight gain and diabetes, highlights crucial issues. If there are wildly effective but very expensive drugs for obesity, suddenly, obesity becomes something we need to avoid.
I've written before about the impact of antipsychotic medicines on obesity (in brief: they are bad1).
We need to address the contributors to the problem we are aware of. Sugar, in everything, is an obvious villain. But medications that change our metabolism are another avoidable cause of harm. If we are both aware of it and can do things to address the suffering we will try to trade effectively and make better choices. You can have a cup of coffee without sugar in it. You can treat depression without increasing the risk of weight gain. These are choices.
Today, I want to highlight a new paper, comparing two antidepressant medications—one old-school, one “more modern.” In a recent study:
[patients were randomized to] fluoxetine 20 mg or vortioxetine 10 mg and recorded [metabolic] parameters at baseline and each visit (4, 8, 12, 16, 20, and 24 weeks).
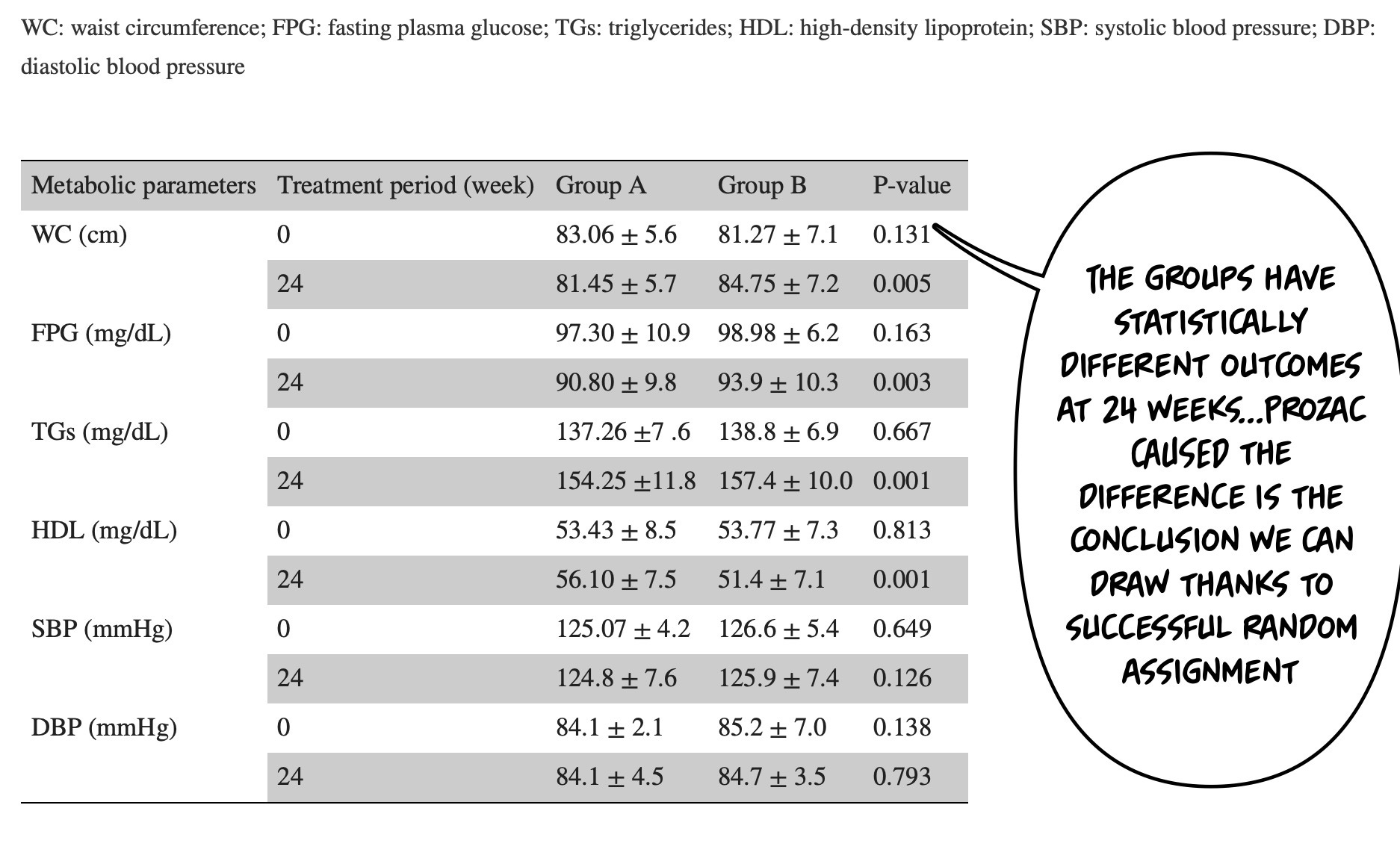
And most metabolic parameters were worse with Prozac:
An independent-sample t-test showed a significant improvement in fasting plasma glucose (FPG) at week eight (p = 0.005), triglycerides (TGs) at week 16 (p = 0.005), high-density lipoprotein (HDL) at week 20 (p = 0.005), and waist circumference at week 24 (p = 0.005) in group A compared to group B2.
As an aside: WHY WOULD YOU WRITE GROUP A VS GROUP B? Write the drug names. Life is confusing enough. moving on…There were no differences in depression outcomes. Blood pressure, also, wasn’t different.
Let’s refresh our “how to know if a paper is bullsh*t skills! We can look at table one!
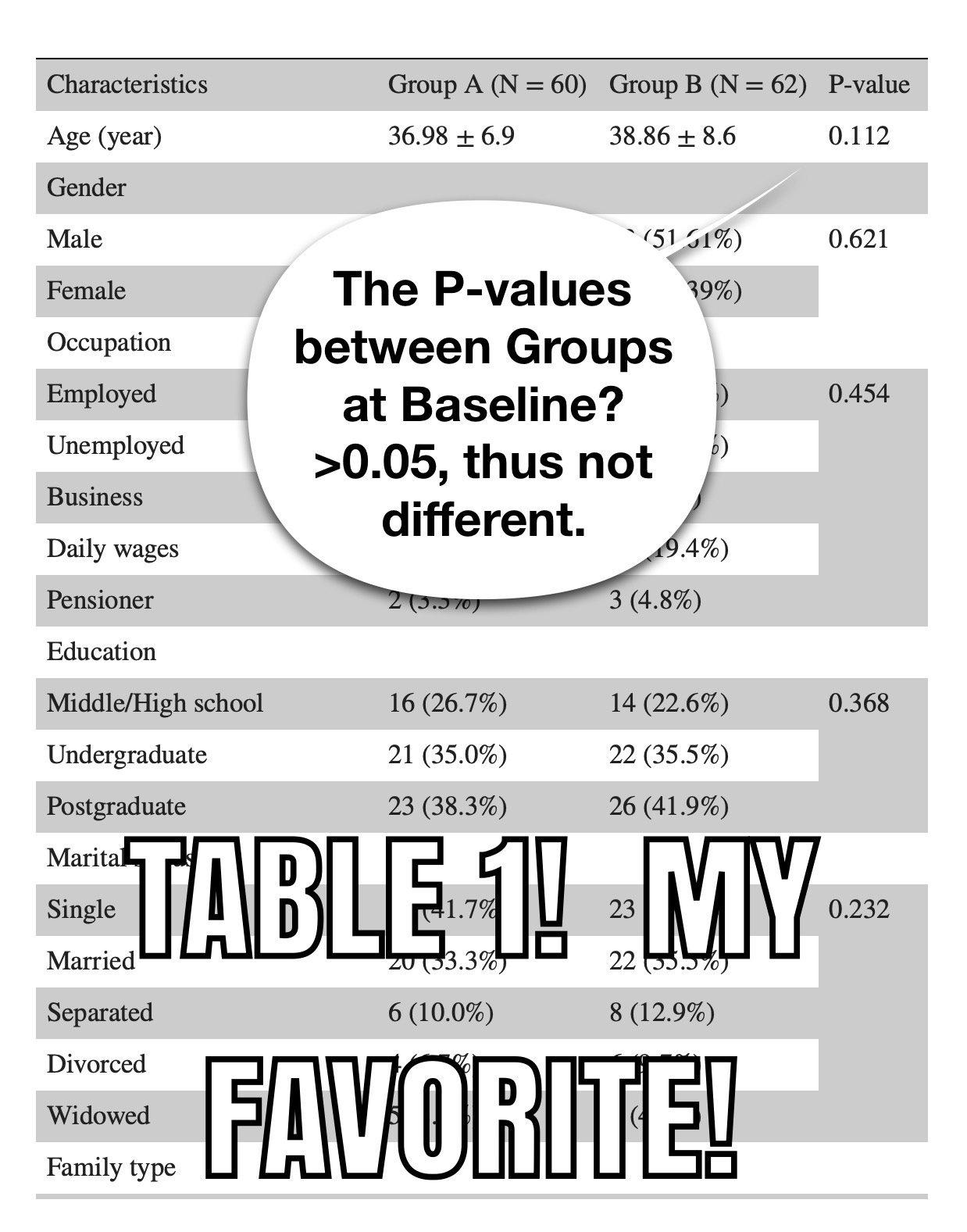
And table one continues…
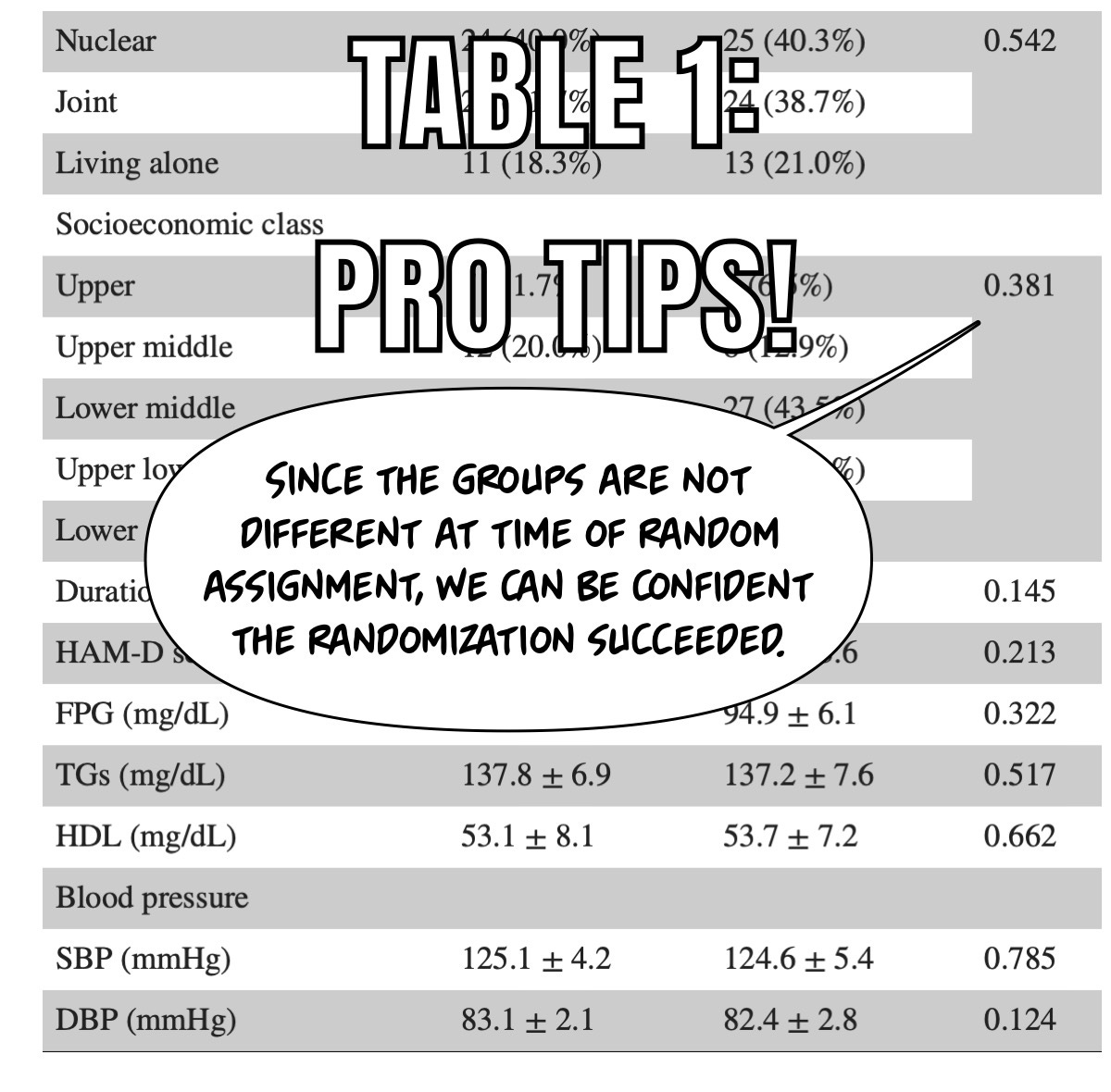
We have successfully randomized the groups. The differences we see at 24 weeks are because of the intervention!
It’s been fashionable to complain about sexual side effects. These are real. However, the severe consequences of whatever PSSD is (as addressed by Awais Aftab in his gracious and humble manner) are relatively rare and not life-threatening. Obesity is life-threatening, over a long enough time scale. It also sucks. SSRI antidepressants are causing it in this study. Depression is a serious life-threatening condition. So it is metabolic syndrome. Let’s take…it…seriously.
Prior articles about how to read science are available to you, my dearest paid subscribers:
How to Read Academic Research Like a (Lazy) Pro
Correll CU, Manu P, Olshanskiy V, Napolitano B, Kane JM, Malhotra AK. Cardiometabolic risk of second-generation antipsychotic medications during first-time use in children and adolescents. JAMA. 2009 Oct 28;302(16):1765-73. doi: 10.1001/jama.2009.1549. Erratum in: JAMA. 2009 Dec 2;302(21):2322. PMID: 19861668; PMCID: PMC3055794.
Sankar K, Mohathasim Billah AA, Shanmugasundram N, Veintramuthu S, Viswanathan S. Effect of Vortioxetine in Comparison to Fluoxetine on Metabolic Parameters in Patients With Depressive Disorder: A Randomized Controlled Trial. Cureus. 2024 Jan 29;16(1):e53178. doi: 10.7759/cureus.53178. PMID: 38420046; PMCID: PMC10901552.
I view this as a real problem. Obesity often contributes to depression and these meds contribute to obesity. We should always pick treatments that are weight neutral or than favor weight loss. Meds that cause weight gain should only be used after a very careful consideration of risks and benefits. I follow this rule in treating cardiometabolic diseases and it definitely helps in that setting.
I put on 35lbs in 6 months on quetiapine. I lost that weight so fast when I stopped the quetiapine that my GP tried convincing me to have an endoscopy as she was worried I had cancer. It was particularly odd because not a single Dr showed any interest when the weight piled on. When my triglycerides came back elevated I was told to eat porridge.
In the UK patients on antipsychotics are supposed to have an annual health check to monitor weight, BP, cholesterol, etc. GP practices receive money from government to do these checks. In reality you are asked to confirm your next of kin. Nothing else. The 1st time my weight was taken was 2 months after I stopped the quetiapine and was due to weight loss.
Unfortunately, about 9 months later I had to swap from pramipexole to pregabalin for RLS and slowly put those 35lbs on across about an 18 month period. I would rather be fat, and the consequences of being fat, than go through the living nightmare that was uncontrolled RLS.