
AACAP Dispatch, Day 2: Don't Break the Blind!
When does blinding matter in clinical trials?

The Frontier Psychiatrists is a daily health-related newsletter. People ask me “what I do” at the child psychiatry conference I attend. I explain that I am a “muckety-muck” and advocate for change. This is not a real job. However, this is one of those articles. I have a real job—seeing patients and running clinical trials at Fermata. We see patients across NY, IL, TX, MA, NJ, CA, and more!
Humans are pattern recognition machines. We are biased toward seeing them. The issue for healthcare and science is that we will imagine patterns with causes regardless of underlying truth.
We also have built-in blinders.
We want to see a pattern. Science uses the opposite bias: we have the null hypothesis— the assumption is that things are not different between intervention and sham or placebo. We say sham in device studies. We are likely to impute difference when there is none.
We use a double-blind design—investigators and the patients should be unaware of random assignment to sham or active treatment groups. This lets us determine causality! Although the double-blind RCT is a brilliant scientific innovation, we should not believe it is always the most appropriate way to answer a question.
My favorite absurdist example is parachutes. Doing a trial between sham parachutes —with enough holes so the person’s fall to their death is not hampered— versus active parachutes would raise eyebrows. There are three excellent reasons for this:
The “placebo response” rate in the condition of “dropping to the ground from a plane” is close to zero.
The ethics of such a study would be highly questionable.
Participants and observers could immediately tell who had been given a sham versus active parachutes.
🪂
The blind would be broken.
Everyone would be able to tell. Furthermore, the actual condition has a fatality rate approaching 100%, and even if the appearance of a parachute versus a parachute is identical, we don't solve the problem of a universally fatal condition with a clever sham control in this condition.
This leaves me my two points for the day:
If the condition never responds to anything other than an active treatment— and there are a few of these that we think, but not none—then blinding and placebo or sham does less to prove a point about a novel treatment than we’d want it to anyway. This is also true in some subgroups across other conditions—depression has a robust placebo response! But highly treatment-resistant depression patients—past about four oral medication trials—have virtually none1.
If the intervention is impossible to misapprehend—everyone will know! Blinding is quixotic. It’s also biasing—in a double-blind placebo trial that is transparently not effectively blinded to anybody, calling it double-blinded makes us think it’s a better study than it is. Simply put, if the blind doesn't make it impossible to tell group assignment because the placebo and the active agent feel enough alike that people can't tell the difference. It's not a double-blind trial.
Yes, I'm looking at you, psychedelic medicines.
What about ADHD?
This makes research data on medical devices like the Monarch eTNS device all the more impressive:
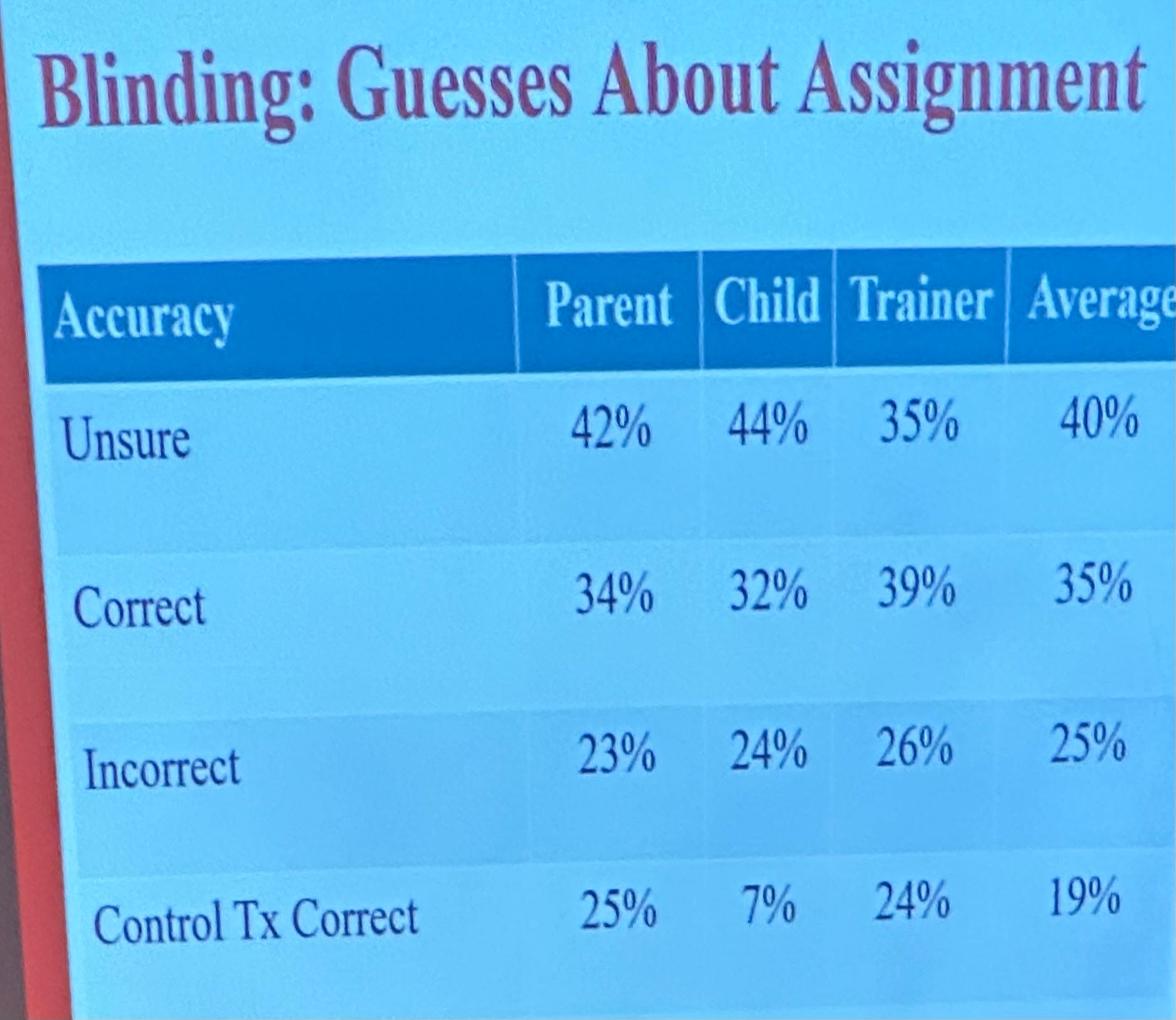
People couldn't, either parents, trainers, or kids, tell which group they were in. This effectively blinded sham control isn't observably different from the active intervention!
Attention deficit hyperactivity disorder (ADHD) has a poor placebo response—even the MTA trial designed to compare therapy to stimulant medicines—was to be stopped early at a midpoint analysis because it was deemed unethical to continue to provide children with an alternative to medication that was so much less effective!
It's the attention equivalent of falling out of a plane. Only real parachutes will do. Brain Stimulation with Monarch eTNS is one such parachute, and the study designs are robust enough to prove it!2
(Yes, we prescribe the Monarch eTNS device at Fermata! Our sister practice in Sunnyvale, CA, Acacia Clinics, also does!)
Reporting from AACAP 2023,
—Owen Muir, M.D.
Disclosure of conflicts—no financial conflicts exist. I am neither a consultant to Neurosigma (the device maker) nor an equity holder. I'm just a fan, prescriber, and user of the device myself.
Cusin C, Colloca L. Treatment-Resistant Depression—Resistant to Placebos as Well? JAMA Netw Open.2021;4(9):e2127952. doi:10.1001/jamanetworkopen.2021.27952
McGough JJ, Sturm A, Cowen J, Tung K, Salgari GC, Leuchter AF, Cook IA, Sugar CA, Loo SK. Double-Blind, Sham-Controlled, Pilot Study of Trigeminal Nerve Stimulation for Attention-Deficit/Hyperactivity Disorder. J Am Acad Child Adolesc Psychiatry. 2019 Apr;58(4):403-411.e3. doi: 10.1016/j.jaac.2018.11.013. Epub 2019 Jan 28. PMID: 30768393; PMCID: PMC6481187.