

Cerebral: Vastly Exceeding the Standard of Care?
Cerebral: Vastly Exceeding the Standard of Care?
And no, that is not praise. A hot take, in seven parts.

Part 1: ”There Have Been Concerning Reports”
Recently, a whole blizzard of reports has come out about the care provided by Cerebral. For the uninitiated, it is the high growth mental health startup. Cerebral raised a hell of a lot of money. This includes financing from Oak, as well as Softbank— of Uber and WeWork infamy.
My hot take? Even based on the most critical reading of what happened at Cerebral— and I’m only relying on already published information— they did a better job than most outpatient mental health care in the United States.
This is not to say Cerebral did a great job. It’s not to defend what happened at Cerebral. It’s not to attack what happened at Cerebral. I don’t actually know what happened at Cerebral.
I do know that, when examined in the context of what happens in outpatient mental health care, it doesn’t look good for the field, but doesn’t look particularly different at Cerebral.
For absolutely full disclosure, I know Dr. David Mou, the current CEO at Cerebral, personally though have no other connections to Cerebral or to its investors.
My wife went to residency with Dr. Mou and worked with him on the inpatient psychiatric ward when he was in medical school. I think it’s important to try to get medical care for psychiatric illness to people who desperately need it. I also think it’s important to do it well. So this is going to be some armchair quarterbacking, but I’m going to try to be fair.
Just before Softbank funded Cerebral, a close psychiatrist colleague interviewed for the position Dr.Mou went on to take, Chief Medical Officer. The only thing I will say about this particular interview, is that she asked one really important question about controlled substance prescribing. It led to her stepping away from the interview process before any non-disclosure agreement was signed: “What are you going to do if the Ryan-Haight Act gets reinstated?”
The Ryan Haight act forbids the prescribing of controlled substances to patients you haven’t ever met in person.
The answer from both the Chief Operating Officer and Kyle Robertson, the slightly-older-than-teenager who was the CEO at the time was the same in independent interviews: “We hope it doesn’t!”
This was not, in case you missed the point, a satisfactory answer.
Part 2: This is Why We Can’t Have Nice Things
Ryan-Haight, as a law, expressly exists to prohibit online-only pill mills.

When Covid hit, the Ryan-Haight Act, out of necessity, was suspended. A series of telehealth companies capitalized on the opportunity to be able to prescribe all of the controlled substances their patients/customers desired by telehealth (or, in some cases, texting) alone.
This includes companies like MindBloom, who prescribe orally compounded ketamine for depression and companies like Done and Cerebral who prescribe stimulant medications to treat ADHD.
So I’m going to take some time looking at the fundamental concerns with this approach, and then we’re gonna dig into the data provided by Cerebral or unearthed by journalists.
Part 3: A Dangerous, Addictive Controlled Substance Similar to Methamphetamine
I am not a bullshit psychiatrist. I am not a reckless drug pusher. I am the author of Adolescent Suicide and Self Injury: Mentalizing Theory and Treatment.
That’s a manual for therapy. I am an MD, and I’m working on therapy manuals. I have hundreds of academic citations, I am the narrator of educational modules on ADHD, I do all the things that respectable academics do and then some.
I’m not the enemy.
I say all this because every time there is any problem with any company that’s doing any prescribing of controlled substances for a psychiatric indication, the sky is always falling. I am no Chicken Little. I have seen a lot of acorns fall and a lot of chickens get eaten in my professional career and so my hot take is a little different.

And so I’m gonna say something very simple: not all controlled substances are evil.
Opiate medications are not good. They’re almost never good. Pushing them on doctors was a scam.
The same cannot be said for stimulants. Every time there’s any reporting on stimulants, journalists are leaning into how these are dangerous and addictive they are.
For good measure they will comment on how Adderall is chemically related to methamphetamine.
This is scaremongering. It’s also stigmatizing, both for people who legitimately take these and other psychiatric medications and for the doctors who prescribe them.
Yes, you can get addicted to Adderall. Yes, that can be dangerous. But some background might be helpful:
Stimulant medications are some of the oldest medications we have in the field of psychiatry, dating back to the use of dexedrine at the Bradley Children’s Hospital in the 1930s.

Attention deficit hyperactivity disorder is a medical condition that is extremely common— about 10% of the population will have it in childhood. I have ADHD. I have taken stimulants for that condition. Left untreated, ADHD is associated with a host of negative lifelong risks beyond bad grades, including more substance use disorders.
I see a psychiatrist. That person prescribed the medication. I never get it from anybody else. Because that would be dumb. I never prescribe it for myself.
Is that defensive enough?
Why did I spend all that time being really defensive about it? Because this is a stigmatized condition. And because of that, we stigmatize its treatment. But now would be a good time to do a deep dive into evidence:
The landmark study on the treatment of ADHD is called the MTA trial, and it was performed at a variety of sites including NYU, where I trained. It was designed to determine if medication and psychotherapy for ADHD were just as good as each other. That is not what the study found. The study was in fact stopped early by the institutional review board because they determined that continuing the trial was unethical. It was not unethical because stimulants are dangerous. It was considered unethical to continue to give children the less effective treatment of psychotherapy alone because they would be harmed by not having access to stimulants if the placebo controlled trial were to continue.
The effect sizes of stimulant medications are huge – and this is a measure of how potent a treatment is, not just if it’s different from a placebo sugar pill.
Part 4: The Science of Weak Sauce
Most of the small molecule drugs we have at our disposal in the field of psychiatry, like Prozac, Zoloft , the usual suspects, are kind of weak sauce. These medications don’t work spectacularly well, and have a risk profile that is relatively safe. But the reason they are so safe and the reason they don’t work all that well is basically the same: these drugs don’t do that much, one way or the other. How do we quantify not doing much? We use the concept of an effect size: how big of a difference are we talking about between this intervention and a placebo or sugar pill?
In the case of SSRI medications in depression for people who’ve never had depression before and are in a research trial because they have literally no other problems, the effect size is around 0.5 standard deviations. This means, to put it in terms most people could understand, the difference between someone have an IQ of 100 and someone having an IQ of 106.5. One standard deviation would be an IQ of 115.
Stimulant medications have an effect size of about 0.8-0.9, and that ends up being about 13 points of IQ if we were making the analogy.
These are big differences for stimulants and not very big differences for antidepressants.
Stimulant medication which include the mixed amphetamine salts, a.k.a. Adderall, that are prescribed by Cerebral clinicians are among the most effective drugs in all of medicine when prescribed to treat ADHD.
It doesn’t mean they should always be prescribed for ADHD. Sometimes the risks and benefits don’t make sense for a particular person. That having been said, these are first line interventions. This is the thing that is the best for treating what can be a really serious and disabling condition.
So that’s my high horse about stimulant medication: they have side effects like every medication. They have risks like every medication. You can get addicted to them if you take too much of them. They can harm you. But unlike opiates, which have almost unlimited harm potential and very little benefit past their immediate ability to relieve postoperative pain, they aren’t medicines that shouldn’t be prescribed or at least offered to people who have the condition that they are good at treating.
Part 5: Mansplaining Organic Chemistry From a Former MCAT Instructor
Just because something is chemically similar does not mean it is anything like the other compound you’re using to scare people. This is intellectually disingenuous at best, and ignorant of how organic chemistry works at worst.
Let me prove it to you: ethanol and methanol differ by only one carbon and two hydrogen molecules.
Ethanol:
Methanol:
Ethanol is chemically similar to methanol. But you can drink ethanol for a night out and have a great goddamn time. If you drink methanol, you will die. You will die because it will poison your liver until it is dead from formic acid poisoning:
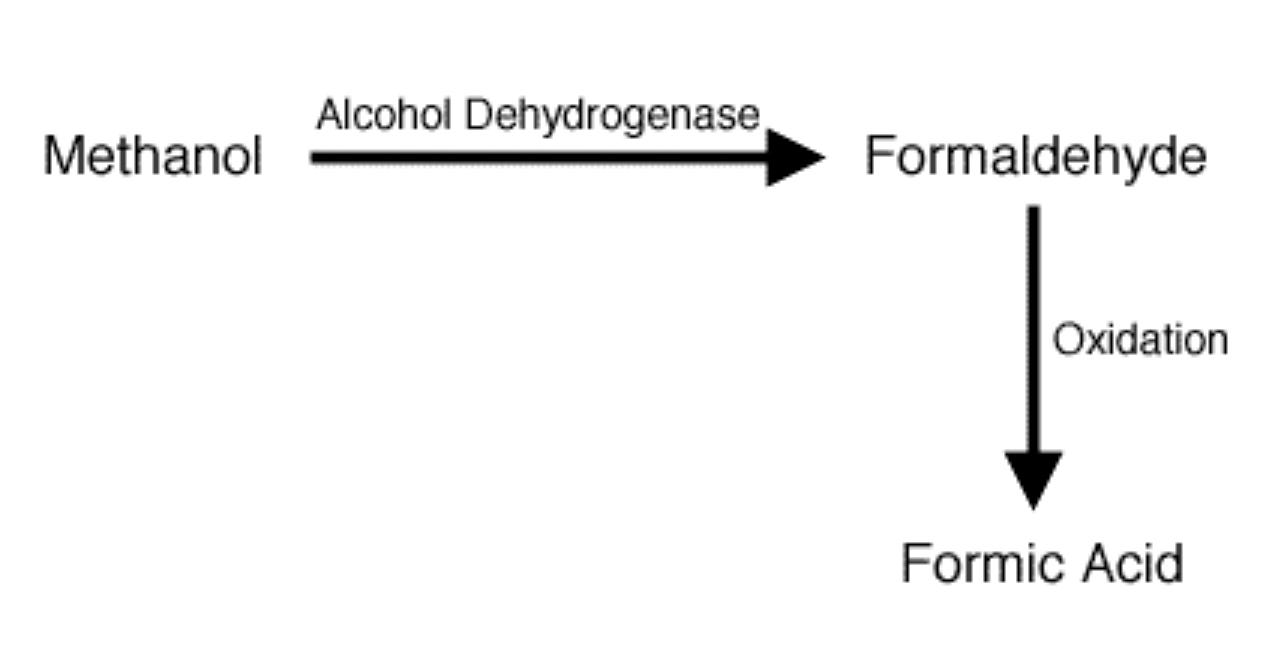
That one carbon and two hydrogen difference in the structure is the difference between life and death.
So based on a lack of understanding of organic chemistry, you can say almost any small molecule such as…
Amphetamine:
Or Methamphetamine:
…is similar to any other small molecule and be saying nothing more than you don’t understand organic chemistry or how those compounds react or interact in the body. And if you don’t understand what you’re talking about, stop talking about it just to scare people and sell publications. It’s irresponsible. Let me illustrate:
One of the most toxic substances on earth is dihydrogen monoxide. It is fatal in overdose, is responsible for thousands of deaths a year, and it’s so addictive that once dependent on it—which can happen in infancy—humans will die within only a week or two of their access being cut off. It is broadly available, with only minimal attempts at regulation, and at the same time in overdose can cause hyponatremia and sudden cardiac death. Dihydrogen monoxide kills, it kills children, it kills old people, it kills dogs who love to frolic in lakes. The menace needs to be stopped.
Dihydrogen monoxide has another common name. Water. Two hydrogen atoms + one oxygen atom. You see what I did there? Yeah, so I’m not gonna belabor the point. Oh wait. I already did.
Part 6: Misleading Statistics, Meet Limited Understanding
Every mental health start up that has high growth gets treated like Theranos when there is a sign of trouble. Leaked documents are the source of much of the data that we are presented with. Much like the Cerebral marketing material, unfortunately none of these documents include information about base rates.
A base rate is how often something happens in the population. So, if I told you that I went to a party and 100% of people were mixing their drinks with compounds containing dangerous dihydrogen monoxide, that would sound like a big deal. Except every time anyone goes to a party and makes a mixed drink, there will be water in it. The base rate is 100%. So the alarming event rate rate in this particular context is identical to the base rate.
With that piece of scientific understanding, let’s jump into what was reported from the leaked documents inside Cerebral:
As reported in Business Insider, there were 2060 incident reports filed by employees in seven months in 2021. Since opening its doors in 2020, Cerebral has treated on the order of 400,000 patients. If we assume something like three visits per patient, which is likely a low estimate, then we are getting to well over 1 million visits over the course of its history. So taking our really conservative estimate, we’re talking about a 0.006% incident report rate per visit.
This is healthcare in America we’re talking about. If there was any single field of medicine that had 0.006% rate of bad things happening I would be jumping up and down. This would be a cause for unbelievable celebration in any context I can imagine.
The best estimates of the rate of medication error in hospital settings are around 8-25%.
About 1.5% of all prescriptions in the community setting have a dispensing error (BMJ Open Quality, 2018).
Dosage errors are the most common type of medication administration errors. 7.8% of carers reported giving an insufficient dose, 6.6% reported giving an overdose, and 5.4% reported giving the wrong medication (PLOS One, 2016).
And that’s just looking at some easily accessible data about medication errors. I think we all agree those numbers are surprisingly high. So before we start losing our mind—get it? – About Cerebral’s rate of incidents reported, we need to keep base rates in mind with treatment-as-usual before the unicorn startups came to town.
Reporting also highlights that Cerebral would enroll patients with complex conditions such as bipolar disorder and sometimes assigned them to clinicians who lacked sufficient training to treat them. This includes psychiatric nurse practitioners and family medicine clinicians.
I actually have no doubt that those concerns are correct. The reason I have no doubt about that is because very few individuals have sufficient training to treat those conditions, and the standard of care is no care. Or insufficient care. Most of the people taking care of most of the mental health conditions are mid-level providers or primary care or both, not psychiatric specialists for complex conditions. It is estimated that primary care clinicians see about 65% of all mental illness cases in the United States. Again. There are only about 30,000 psychiatrists in the United States in total, and there are easily 5.7 million individuals with diagnosed bipolar disorder for that inadequately small workforce. Keep in mind there is a total of about 60 million adults and children in the U.S. with a mental illness at any point in time.
This is a huge problem. But it’s not a problem Cerebral can solve even with the most aggressive messages from bubbly recruiters on LinkedIn. If there were enough people to hire, on earth, I imagine they would do it. They have $462 million with which to pull that off. I doubt it’s for lack of trying.
They reported that staff at Cerebral could use a Google Form and a Slack channel to report incidents outside the normal course of business. It seems highly dismissive to say that this is all they did. I’ve worked in a lot of healthcare settings, and having a Google form and a Slack channel you could put concerns into is technology light-years ahead of what is available in almost every hospital. It’s like a machine that allows time travel in comparison to the technology accessible to most outpatient clinics who still fax things to each other. Even having the ability to track incidents is so foreign to most outpatient medical care and mental health care it boggles the mind. If you call up a private practice psychiatrist and ask how many incidents they logged in the past year, they probably would tell you that you had the wrong number (if they even actually answered the phone).
Inability to track absolutely anything at all is one of the reasons my wife went to work for Osmind, which is a healthtech company that strives to enable mental health clinicians to be able to perform the kind of tracking that Cerebral is reporting on and act accordingly. The fact that they are collecting and analyzing these numbers is a success. The fact that they’re not perfect is above par for the course.
Consider that every licensed provider Cerebral hired at some point got that license. It’s those trained and licensed individuals who are out there doing something, presumably practicing medicine or advanced practice nursing or therapy before they got to Cerebral. And every single one of the incidents reported was done by someone who was unable to be tracked previously, and after they leave Cerebral are highly unlikely to have their practice tracked thereafter.
But they were treating patients. And they probably still are treating patients. They’re probably charging more now after leaving Cerebral and many will not continue to take insurance in solo practice.
Now lest this were to sound like defense of Cerebral or even equivalence with some thing that we should be happy with, it’s not.
Neglect, misdiagnosis, regulatory noncompliance, and bad outcomes with unhappy patients is not even the status quo. The status quo is no care at all, particularly for those with serious illnesses. It is estimated that nearly half of the 60 million people with mental illness in the U.S. go without any treatment. One of the things David Mou, currently the CEO at Cerebral and previously their Chief Medical Officer emphasizes is that many of the people getting care through Cerebral have never had mental health care before.
I believe the term he used was Cerebral had the privilege to care for these individuals. These are people without means to access fancy pants doctors like myself.
This is the bottom of the barrel we are, collectively, scraping. This social barrel is one in which common, disabling, and in some cases life-threatening illnesses are so horrendously under addressed that the first time many people got access to anything that resembled healthcare was a startup founded by someone with no healthcare experience and a non-psychiatrist physician cofounder who had his medical license reprimanded for prescribing medications without proper examination at a prior startup. At least now, a well-trained psychiatrist and full fledged grownup is at the helm.
Part 7: Perfect is the Enemy of the Good
People were blown away by Cerebral‘s traction. I wasn’t. They offered something that was desperately needed and not available: the ability to book an appointment with a mental health professional who took your insurance—and get one in a timely fashion.
It is noted that 50% of the patients who sought care with Cerebral who were suicidal at the time were no longer suicidal six months later.
There are two major problems here, and a third implied by the others. The first problem is that we don’t know the base rate of suicidality in either this population or in any population. We know it’s absurdly high. We don’t know how many of those individuals would’ve killed themselves without treatment.
We also don’t know if 50% of people in six months no longer being suicidal is a success or a failure, compared to whatever the natural course of suicidality waxing and waning might be.
But the thing that is most striking is that none of those patients would’ve been able to receive care at almost any private practice in the city in which I live, New York, if they were honest in calling around to find someone taking new patients (yes, calling because that’s typically how it is still done in private practice). If you’re suicidal, you get turned away from most private practices in the city (which of course don’t accept your expensive insurance either!). Cerebral chose to treat these individuals. Some of them benefited from that treatment. Some of them would’ve gotten better anyway. Absent Cerebral, likely all of them would have been up shit’s creek, and none of us would’ve known about it.
I am arguing the tools did not exist and do not exist for Cerebral to accomplish what it attempted. Any technology that would be needed to track and predict such outcomes has to be built from scratch or repurposed from goddamn Google Forms.
I am also arguing that the professionals that would’ve been necessary to treat these individuals are too busy not doing so because they’re stuck on the phone with United healthcare doing a prior authorization, or thinking about killing themselves quietly because they’re so burned out, or working in an inpatient psych unit which may even increase the rate of completed suicide over the long term as far as any of the data can tell us.
There are not enough experts for people suffering even at the scale of an additional 400,000 coming to care in the United States. The professionals don’t exist. The tools don’t exist. The treatments don’t work well enough. The one problem that they did robustly address, ADHD, was a smashing success from a marketing standpoint. And from a customer retention standpoint. And the insinuation from the media is routinely that’s because addictive drugs were handed out and people got hooked or had bad reactions. And that’s almost certainly true for some of those individuals.
It is also possible that thousands of people got almost immediate access to the first line treatment for their condition, if it was ADHD, and found it so helpful that they routinely made follow-up appointments to get that controlled substance refilled by a licensed prescribing clinician. It may not be the substance they were addicted to- it may have been feeling better because the first line treatments for that condition are miles better than the first line treatments for any other conditions we have in common usage. Let’s not forget that untreated ADHD is associated with higher rates of substance use, car crashes, underemployment and even divorce.
Cerebral had the temerity to both raise money to take care of people who didn’t have great insurance or unlimited means, who watch TikTok, and who are suffering.
And all of a sudden everyone really cares about how much they’re suffering because 12 of them have a bad outcome, or 2060 of them had an incident report.
That’s news.
But the people who are suffering before Cerebral, the people who are suicidal, the people who are mentally ill, and seriously so, are still suffering now. Cerebral may have changed it for some of them, but they dared to advertise, and do an imperfect job that we don’t know the full scope of, but I find it hard to believe the argument that’s worse than the absolutely nothing that so many of us, even the privileged, are left to struggle with.
We yearn for the perfectly safe, the well executed, the slowly deployed, and all of this is deemed to be more important than helping people who need help now.
Cerebral is an easy target. Cerebral is guilty of trying to help the mentally ill using economies of scale in a way that was new for a fragmented and wasteful mental health system that no one thinks was doing anything close to a good job before Softbank showed up. Cerebral may be guilty of a variety of regulatory and other missteps or crimes—we will find out soon enough. However, exercising restraint in sloppy critiques of overly ambitious young people and well-meaning clinicians—who were trying to disassemble the fire pits in which young people immolate themselves—is a virtue.
We should perhaps be a bit more mindful of the gawking and peanut crunching we do when surveying the wreckage of the lives of others. Particularly when our track record in the same endeavors—and in our healthcare system overall—is worse, not better, than anything in these leaked incident reports.

Building a better mental health care system requires coordinated efforts across technologists, clinicians, patients, investors, payers and regulators to make the standard of care something we are not embarrassed about. Worrying about the sky falling over stimulant prescriptions misses the point that the very foundation of our mental care system is built on quicksand.
With great appreciation to those who read this far, and understanding for those whose depression or inattention got in the way of finishing this article…
—O. Scott Muir, M.D.
This is a good piece — writer is a good and sharp thinker and he is good at criticizing the system while neither exonerating nor alienating himself from it, which is a trick few people can pull off. The shrinkage world needs a lot more like him.
thank you - great piece