

We Made Inpatient Psychiatric Treatment Suck Less with this One Weird Trick
We Made Inpatient Psychiatric Treatment Suck Less with this One Weird Trick
It is all about how care is paid for.

I know what you're thinking. Because I'm a psychiatrist, and we're psychic. That's a joke. Readers of this newsletter anxiously await the next regulatory issue, on which I will reliably advocate for compliance or public comment to regulators.

Today, the fans of “frontier-psychiatrists-brand public comment” are the winners. We have a real doozy on tap. You have the opportunity to make a big change. Psychiatric and general medical care in hospitals are paid for in completely different ways. In fact, there are two different payment models for psychiatric hospitals on the financial backend. Which contract the hospital has tells you a lot about the incentives they have to deploy novel treatments.
In every other medical condition, the payment model follows the same basic principles: you may get a hospital bill, and it's got a bunch of line items, and it's for a phenomenal amount of money, and then it gets knocked down to this or that. The mystery? This is not how any bills from Medicare or other payers are paid. The bill you see is fiction…if you have insurance. The song and dance are all there to obscure the fact that everything is paid differently. The first system—and to be clear, this is the better one— is the DRG system, which has its own associated contracts.
Diagnosis-Related Group (DRG): Under the DRG system, patients are classified based on primary ICD-10 diagnostic code, surgical procedures, age, etc. Each DRG group has a fixed reimbursement rate. Hospitals receive a single payment per patient per DRG. This system “encourages efficiency and cost containment,1” but at least it is internally consistent. It’s the prix fix menu approach to hospital payments.
So, for medical hospitalizations, they're getting a lump sum. The hospital has every incentive to take care of you in the most cost-efficient manner, and they get some adjustments to how much they get paid based on how much it's likely to cost. All of the negotiations are around the multiplier the hospital gets for the management of any given DRG in their setting. These multipliers for any DRG payment are considered proprietary by third-party payers. 2
Most psychiatric hospitals don't work this way. There are two different models with two different fee structures:
Per Diem: Under the per diem system, hospitals receive a daily rate for each day a patient is in the facility. This rate covers care costs, including room and board, nursing care, and other services. They get paid more for longer stays, and the risk is that insurance will stop paying on individuals the doctors don’t feel safe discharging, and the hospital has to eat the cost.
Inpatient Psychiatric Facility Prospective Payment System (IPF PPS): The IPF PPS is a Medicare payment system specifically designed for inpatient psychiatric facilities. Similar to the DRG system, it determines payment rates based on a patient's diagnosis, age, and other factors.
There was no financial mechanism to pay for innovative treatment in psychiatric hospitals…until now.
General medical hospitals have a bunch of payments factored into the care of a heart failure patient. That care can involve MRI scanners, surgical interventions, Extracorporeal Membrane Oxygenation, and associated wizardry of modern medicine. If you come into the hospital with a heart attack, they factor in the cost of the cardiac catheterization lab that will save your life. If you need a heart transplant or a heart implant, that is DRG 001. This has a “relative weight” of 28.9651, which is multiplied by a contracted rate, and according to Optum’s guide, has a base rate of $170,646.44 under Medicare.
Until the 2024 CMS update—which inspired this article—the separate billing schemes for psychiatry never imagined any technology being brought to inpatient psychiatric care. When I previously complained about the archaic nature of inpatient psychiatry, even the admittedly nerdy healthcare economics enthusiast author of this column did not know these were different systems from a payment standpoint, much less two separate systems.
The practical upshot? The whole game for hospitals is about getting the most financially viable care per patient. The healthcare payers had the incentive to deny days. Inpatient psychiatry was not motivated to get the person out the door quickly, efficiently, and well.
Enter New Technology Add-On Payments!
If you're reading this, you probably saw that coming! Is he about to mention transcranial magnetic stimulation (TMS)? Is he going to mention accelerated TMS? Will there be a brain scan involved? Will Owen suggest Nolan Ryan Williams, M.D., receive a Nobel prize?3
Dear readers, if you guessed yes, you have correctly identified my emotional conflict of interest. It is now time to support more breakthrough treatments paid for in more psychiatric hospitals. And encourage your local hospital to start incorporating breakthrough treatments into its behavioral health care pathways.
It's a fine time to tell the world that the SAINT neuromodulation system is commercially available. It's an excellent time for anybody to ask their health plan if this is covered under their plan in the outpatient setting? There are new Category III CPT Codes for that, after all.
In a hospital setting, if you're paid to keep people longer, it's hard to understand why you would use a treatment that would get them out faster. Especially if it costs more and you don't get paid more. This is why Per Diem contracting is so pernicious. It doesn't matter how good your intentions are if you're going to financially cripple, your hospital setting, or at least you're afraid you will; it's really hard to imagine you're gonna adopt some novel treatment that will reduce the number of paid days in your hospital. However, if your setting is paid a bundled amount, like every other hospital, stay because your hospital uses the IPF PPS contracting system, and there is an add-on payment to account for the cost of treatment like SAINT —the New Technology Add-on Payment system (NTAP) under medicare—it makes all the financial sense in the world to do the new thing. You get paid more. You probably get the patient out the door faster. That's better for them, and it's better for your hospital financially.
It's completely bonkers that rapid-acting treatments like SAINT are much easier to access in the outpatient setting than they are in the inpatient hospital setting. You should go to a hospital because you have a problem that's really severe, and hospitals can access even more technologies and treatments to keep you alive and get you well. But right now, you can get sent to an outpatient clinic, like Fermata in New York or Acacia Clinics in California, but not in most hospitals. That is beginning to change—MUSC, for example, has one of its hospital's first comercial Magnus Medical SAINT systems.
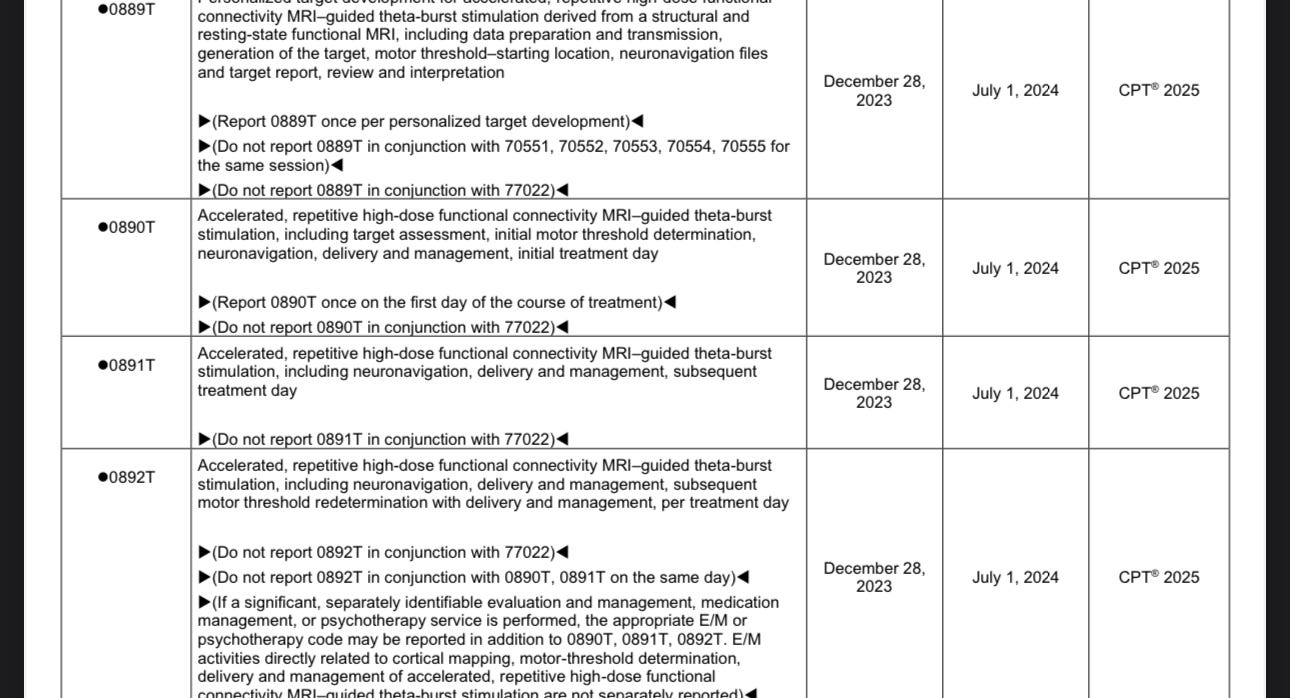
Psychedelic medicines are likely going to need to follow a similar path to payment in the hospital setting. We can all help this happen. Ask the question—in writing—if your plan covers fMRI-guided Accelerated Neuromodulation. Here are the CPT codes to inquire about—they go into effect on July 1st!
If you are near a hospital, ask if they have SAINT for their psychiatric inpatients. If they answer no, send them some fine articles on the topic. Make yourself a bit of a pest. There is no other way they will hear about it that you can count on as much what you are saying directly to them.
So much cost containment. It’s wonderful to see how well it works
This is the kind of thing that legally needs to be public. By the way, any decent machine learning engineer can back-solve DRG multipliers based on claims data. So, good luck keeping that Private and proprietary.
When do I not suggest Dr. Williams receive the 2025 Nobel prize in medicine?
Thanks for the CPT codes. Remember what Arlo Guthrie said: "Three people, and it's a movement."
One additional question that you didn’t mention: Is Nolan Ryan Williams, MD named after the famous pitcher, Nolan Ryan?