

September, 11th
September, 11th
The sacrifices our warriors make for us.

I graduated college in 2001. I remember that day. Many other people remember that day. It has become an anchor, but maybe not the kind we expected. It was the end of peace, and the modern, at least the US military is concerned. The global war on terror created an operational tempo that was not the same as before that day. That operational tempo has continued for many of our special operations forces. Special operations warriors are asked to do things that no one else can do, and they do them routinely because that's their job.
Most of these warriors enlisted after September 11, 2001. Now, service members with 20 years of service enlisted after they knew they were signing up. This was the end of “summer” and the beginning of a protracted winter for service members compared to the rest of America. Most of us will remember Covid-19 as something that changed the world. For the military, it was September 11.
There are new injuries from this conflict. There are far fewer deaths, making it less evident that a war is going on. There is a saying about war: “The only winner is medicine.”
We have learned lessons of the past and learned more about saving people from gunshots, improvised explosives, and other massive and life-altering injuries than we were ever able to before. The casualties are incredibly high in these conflicts. The casualties are also extremely high due to the operational training required for these remarkable missions against asymmetrical adversaries.
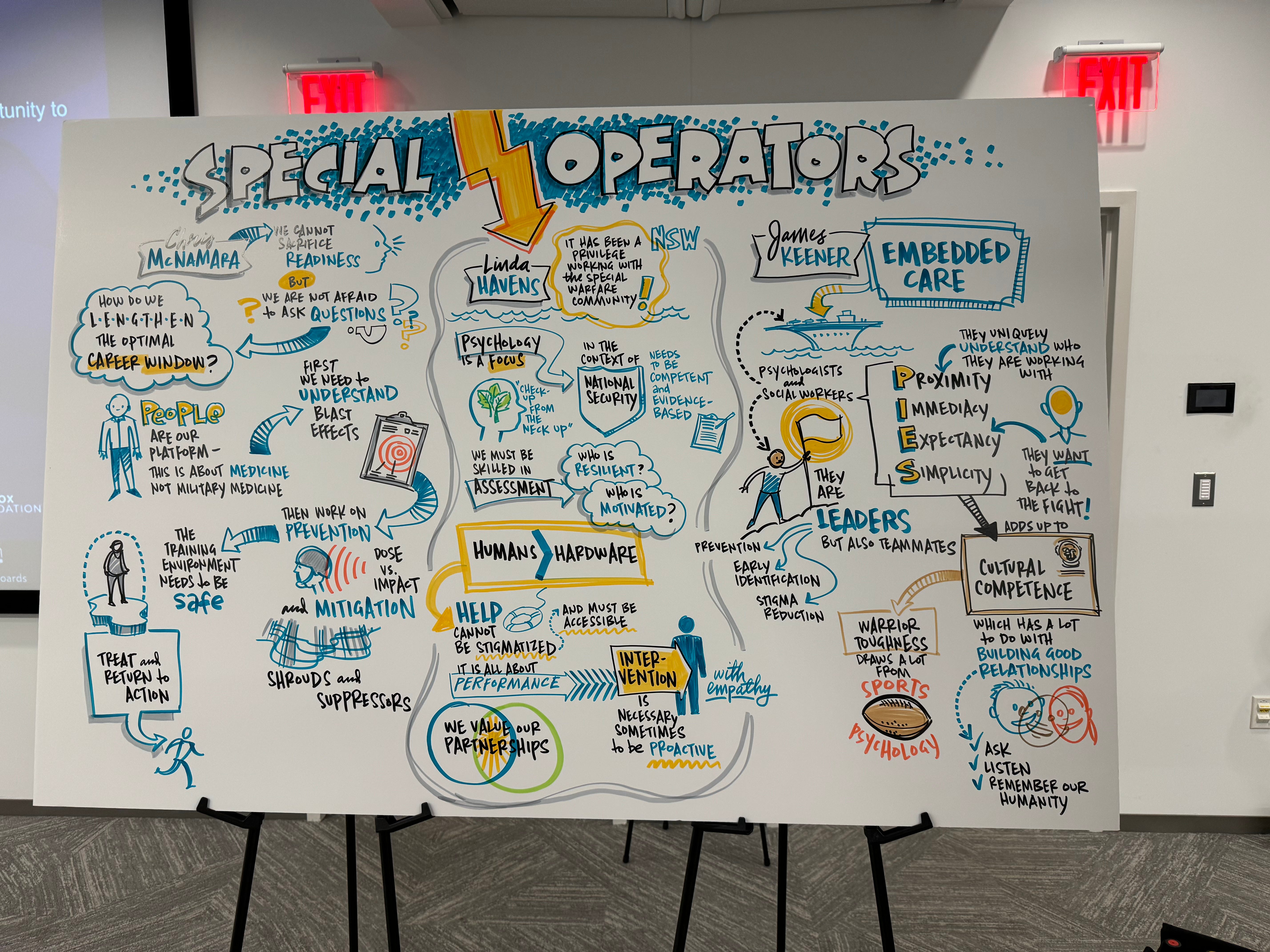
Today, I had the pleasure of being welcomed at Homebase in Boston. Homebase is a collaboration between Massachusetts General Hospital and the Boston Red Sox Foundation and provides neuropsychiatric services to special operations forces, and their families. It's not part of the VA, it's not paid by insurance— it's all grant-funded. Multimodal care, research, and treatment aim to create the most excellent care our Warfighters could want.
I'm going to write about one of those hidden wounds. This will not be about Post-traumatic stress disorder. That's obvious. We all get the veterans get PTSD.
By the way, I'm saying Warrior and warfighter because I am following the custom—soldier refers to somebody who is in the army, marine refers to a marine, airman relates to someone in the air force, and sailor—or sometimes just SEAL—refers to somebody in the Navy. These services contribute warriors to our special operations command, but once you're a special operator, you are the weapon system. There's less boundary between services—the deployments can consist of service members from across branches of the military times, so it's easier to stay warrior to encompass everyone.
These remarkable humans have learned how to fight in a way that maintains their ability to be incomprehensibly lethal. They are not always ordered to kill, they have rules engagement that are much more robust than our domestic police forces. They have lawyers dictating what they can do on the battlefield. But sometimes, warriors kill.
While doing their job, they get blown up a lot. There's a specific kind of injury from being exposed to blasts. Common parlance includes the term “chronic traumatic encephalopathy,” which is the kind of brain injury that people in the NFL have been reported to get from repeated concussion. That's a different kind of injury, pathophysiologically, than what is present in warfighters. They get concussion injuries as well, but a lot of the wounds to their brain have to do with sound waves.
These sound waves are because they're standing next to mortars and tanks, holding rifles, blowing open doors, getting hit with improvised explosive devices, and crucially, they experience all of this in training missions as well.
In training, they jump out of helicopters, ride on fast boats, shoot live ammunition, and practice. They get good at their job. They get ready to fight a war well before they fight the war. To be able to get up in the middle of the night and ship out in under three hours, to accomplish the impossible anywhere in the world, it turns out that it takes a lot of practice. And that practice exposed them to blast trauma to their brain and body as well.
We have a specific name for this. It’s called repeated blast exposure. Ironically, it's similar to the shell shock that we named in World War I, which we assumed wasn't that. The scholarship has advanced, and the medical understanding is coming along with it:
Thanks to the scholarship, we now know there are differences between the injuries sustained from getting hit in the head and having the concussive force of sound pressure waves shaking the brain inside your head. Helmets that were supposed to protect you from shrapnel, thanks to reverb within the helmet, might also make you more likely to sustain this sort of injury. There's a lot we need to learn. Mitigating risk needs to include maintaining lethality.
The risk of suicide in warriors is high. Some of these suicides are from psychiatric illnesses, but in the special operations community, these lesions in their brain have distinct pathophysiology, and like all physical illnesses, they predispose individuals to suicide. Yes, that's right, all physical disease makes you more likely to die by suicide. It's not just mental illness, it's physical illness too. Brain injuries are more likely to die by suicide, also.
Our Warriors have undertaken dangerous careers. That's well-known to anybody who signs up to be a serious warrior. It's our job, as a society, to fund the science and medicine that will protect them from harm to the degree possible and heal them when they hurt. Most importantly, we need to understand their culture and the sacrifices they've made to understand their injuries appropriately in their context.
The world changed on 9/11, but for some of us, the changes were more profound than others.