Welcome to The Frontier Psychiatrists, among the more regularly published health-themed newsletters on the internet. This article is a team effort. It starts with thoughts by Owen Scott Muir, M.D., DFAACAP, (OM) and includes thoughts from David Carreon, M.D. (DC).
OM: I recently flew back and forth to London. My wife was asleep on me for much of the flight there, which made writing less of what was happening. Instead, I watched the Hunger Games movies back to back, all four of them. These are way better movies than I remembered. They also hold together better together than separately, separated by years.
In The Hunger Games, a malicious and Machiavellian government in a central capital decides to keep its 12 out-lying districts in line by “reaping” one boy and one girl from each of the districts and having them kill each other on live TV until there's only one surviving Victor. This is done every year. In short, children murdering children for political sport was the conceit, and the children in question developed Post-Traumatic Stress Disorder (PTSD) symptoms from it.
When I started writing this article, I was planning on arguing what we see in The Hunger Games? It is a dramatic minimization of what 20% of girls and about 5% of boys experience in the United States as sequelae of childhood sexual abuse alone.
When we add broad exposure to mass gun violence, which is now the number one leading cause of death for children in the United States? More trauma. And then you add death by overdose and suicide? I could blame the crisis on trauma at scale. This would validate my preconceived ideas. However, the data I just reviewed and will share with you? It doesn’t support this argument. The trauma is pervasive and awful, but very large-scale data tells a different tale, when it comes to suicide risk. The reaping we have built for ourselves? One in which teenagers reap themselves into oblivion? It’s a catastrophe, to be sure. But exposure to frank trauma isn’t the most significant risk for this tidal wave of death by suicide. This article is about the most horrifying predictor of death by suicide and suicide attempt, which comes to light in a remarkable paper about models to predict suicide.
I’ve written before, as have many, about the mental health crisis…crisis. In summary, my argument is that to call something a “crisis”—for example, the rate of increasing suicidal ideation among teenagers and subsequent death by suicide—is to gloss over the factors driving that very crisis. A crisis is a fine frame to get people out of the path of wildfires. All they need to do is RUN in a direction AWAY from being burned alive! That mission is, thusly, accomplished. The same can not be said for the catastrophe of concomitant sadness, angst, horror, disconnection, and trauma experienced by children today. I am officially petitioning the internet to adopt a new phrase:
“The Mental Health Catastrophe”
Instead of “crisis.” Walking us back from the ledge of invective, I will proceed to ground us in data—this time, at a massive scale. A new article, published in JAMA Psychiatry, is an excellent reminder of the depths of our failure, as a society, to protect children from the nightmare we’ve created.
This study, published just this week, used EHR records…
The original model was a logistic regression… in a sample of 10 275 853 specialty mental health outpatient visits from 2009 to 2015 in 7 health systems, and adapted to a cohort of 1 408 682 mental health outpatient visits at K[aiser Northern California]
to train a machine-learning model in order to predict:
Suicide attempts (including completed suicides) within 90 days of the appointment, determined by diagnostic codes and government databases. All predictors were extracted from electronic health records.1
Based on a sample of mental health intake appointment. I’ve worked on ML models using a combination of biometrics and health record data2, and I promise this is non-trivial work. It’s also worth recalling—health records have only the tiniest sliver of the data that matters the most.
This data is only from mental health visits. It was evaluated post-pandemic:
Data were extracted and analyzed from August 9, 2022, to July 31, 2023.
Their prediction model was relatively accurate…
The model had an area under the receiver operating characteristic curve of 0.77 (95% CI, 0.76-0.78)
This “area under the curve”— “AUC” for short— metric is a broad perspective of the Machine Learning model's performance. A model with perfect discriminative ability will have an AUC of 1, while a model with no discriminative power will have an AUC of 0.5. This model predicted almost half of the subsequent suicide attempts in the population:
The 10% of appointments at the highest risk level accounted for 48.8% (95% CI, 47.0%-50.6%) of the appointments followed by a suicide attempt.
Suicide is a rare outcome. Suicide attempts are less rare, by definition. The fact that basic demographic information and the notes your doctor makes can identify risk is helpful to know, but its utility depends, of course, on what action can be taken to avert the catastrophic outcome of a suicide attempt or, heaven forbid, completed suicide. This sample has the scientific virtue and the deeply humbling reality of capturing some death by suicide:
There were 2800 scheduled appointments (0.17%) that were followed by a suicide attempt within 90 days. At the patient level, 2023 unique patients (0.24%) had a suicide at- tempt, and 78 of these attempts (3.9%) were fatal.
The authors were building a machine learning model to determine what factors predicted death by suicide in their population. To be clear, most science is about “samples,” in which we are only looking at a subset of a population. This data from the massive Northern California Kaiser health system includes their entire population. It’s not a sample of that cohort—it’s everyone. The covered population in this area includes Silicon Valley.
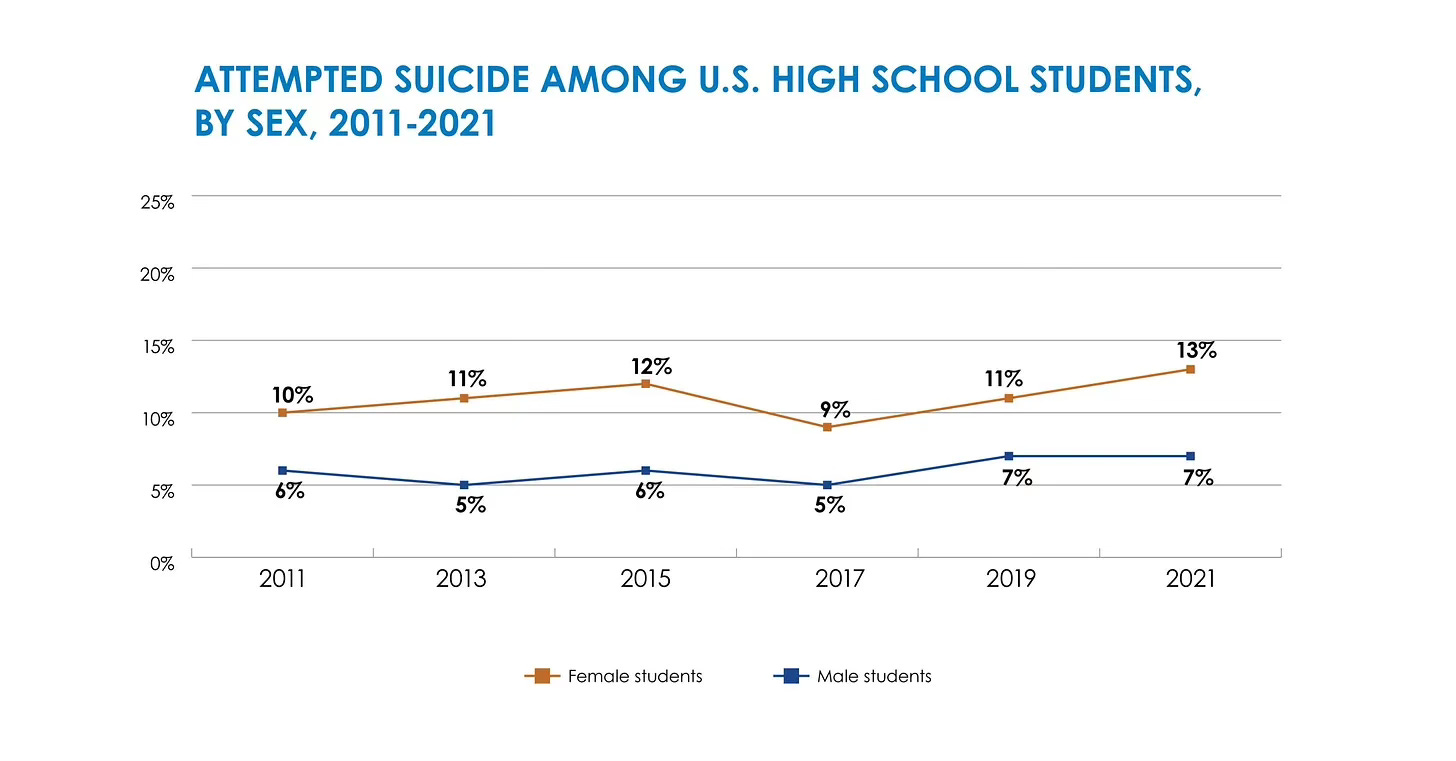
It’s worth reminding readers, according to the CDC, the rate of suicidal ideation, attempt and completion has been on the rise for everyone, but particularly young girls (quoting from this very newsletter):
Nearly 1 in 3 (30%) seriously considered attempting suicide—up nearly 60% from a decade ago.
Attempts to die are up as well, with just under twice as many girls attempting to end their lives in high school as boys:
A total of 49,449 Americans died by suicide in 2022, the Centers for Disease Control and Prevention said Thursday.
This is a 2.6% increase from 48,183 in 2021 and the highest number ever recorded, according to provisional numbers released in a new report from the federal health agency.
It is at this point I will pass the mic to David Carreon, M.D., for what we learned from this population-level data—some of which means physicians have to unlearn what we were taught in medical school, at least if we happen to be practicing in Northern California.
DC: It turns out that medical school was wrong. Or at least it became wrong. Suicide is notoriously difficult to predict. Many factors go into this devastating outcome. As psychiatrists, we have the unenviable job of deciding who’s “high risk.” We learn acronyms in medical school to help us remember the risk factors (e.g. SAD PERSONS3). It was assumed that these were stable “risk factors,” like smoking is a risk factor (and cause) for lung cancer.
S – Sex = male A – Age (<19 or >45 years) D – Depression P – Previous attempt E – Excess alcohol or substance use R – Rational thinking loss S – Social support lacking O – Organize Plan (with which one could end their lives) N – No Spouse
S - Sickness (physical)
That data from Papini et. al., however, presents an unsettlingly different picture of risk. Recall, that their endpoint was defined as follows:
The outcome was defined as suicide attempt at any point 1 to 90 days after the date of the scheduled intake appointment. To be consistent with the original model, suicide attempts also included completed suicides.
The authors note there were no differences in the prediction of attempt and death by suicide. The attempters and the dead looked, from a data perspective, identical.
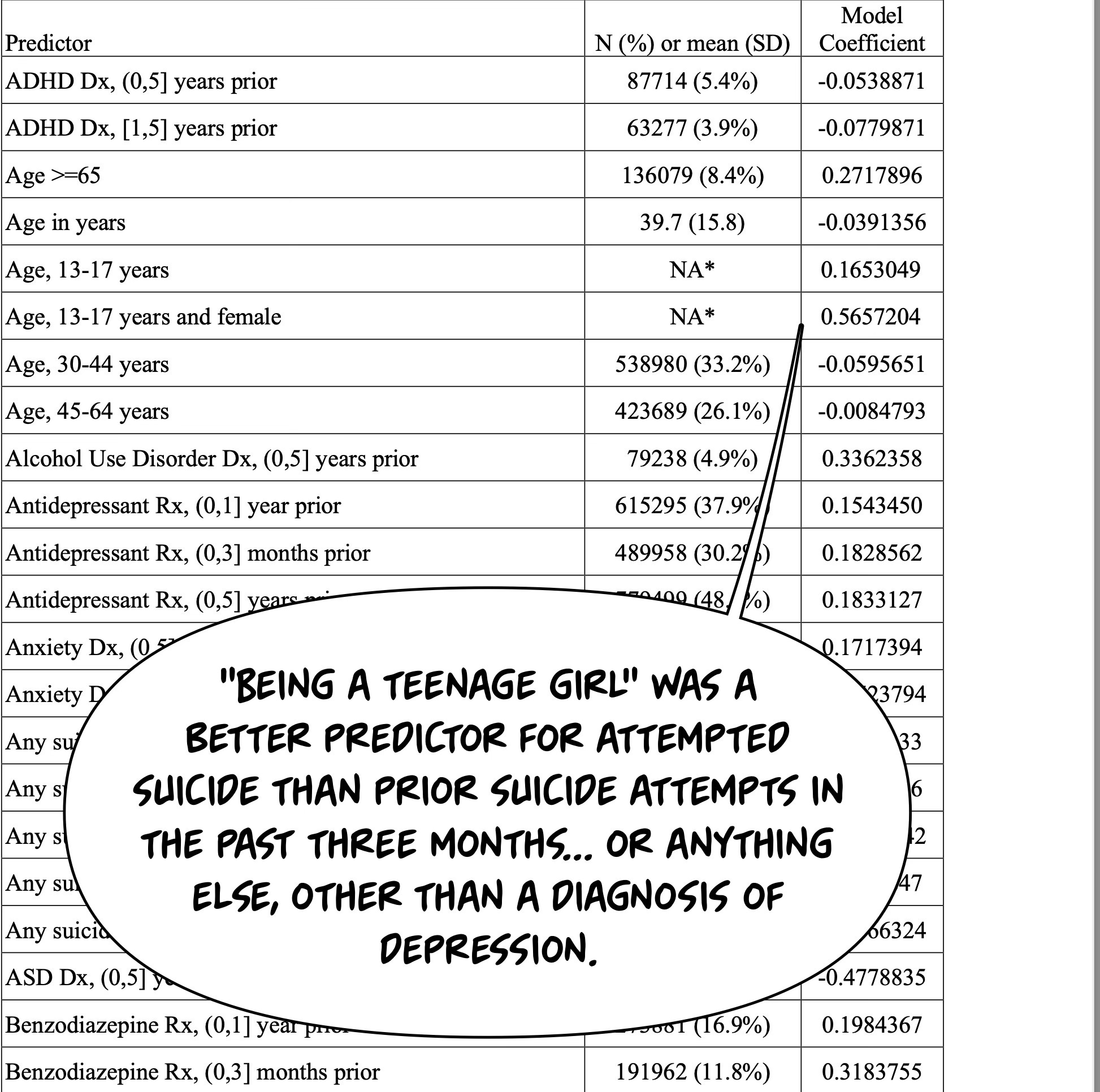
In this sample, the strongest predictor of death by suicide was a depression diagnosis at intake. That isn’t surprising, I suppose. What is vastly more unsettling is the predictive power of the second-most predictive variable. It was a demographic factor.
The highest demographic risk factor? Simply, it was being a girl between 13 and 17 years old.
OM: Hold on a minute…what about traditional risk factors like having previously attempted suicide? Or a recent suicide attempt in the past three months? Or Drug Abuse? How about my precious theory that it’s trauma, like in The Hunger Games, messing kids up?
DC: These factors, after depression, were all less predictive of suicide attempt or death than existing as a girl between the ages of 13-17. I checked and rechecked the table. Maybe it was like golf? In that game, you want a smaller number. Or maybe I got the sign wrong. I checked a few other typical predictions – and they were all there, right from what I learned with SAD PERSONS. Recent suicide attempt? This predicts suicide completion. Recent hospitalization? Check, this also predicts suicide completion. As has been covered here, recent benzodiazepine prescription predicts suicide (though notably most predictive when a person had been trying one for three months, more than one or >3).
No. Nothing was wrong with my math. Nothing was wrong with the authors’ math. The lethality of being an adolescent girl? It is just a fact in our modern era.
There is something I love about registry studies. They’re not exactly science. Or, more accurately, they’re better than science. A census doesn’t try to estimate the population. Your tax accountant doesn’t “model” your finances. Your gas station attendant doesn’t make a data-driven, machine-learning prediction of the number of candy bars you buy and then charge you the predicted price. They count. It’s not science; it’s math. And with registry studies, you have not just a “representative sample” of the data. You have all the data.
There are, of course, areas of uncertainty. The registry may be lacking. Or it may not be true of other registries. Or it may not be accurate in the future. But at the time of the study, it is as close to the ground truth as you can get, free from many biases inherent to science and scientists with their penchant for samples.
It’s very dangerous to be a teenage girl in Silicon Valley. As a long-time physician caring for those in our Valley, we are a beacon of technologic hope. Today, I drove past the Tesla Factory. I just treated a Microsoft engineer. I’m writing this on a MacBook Pro, designed in Cupertino, California, a single-digit number of minutes drive from where I work.
How did it happen that, in the space of a decade or two, one of the lowest suicide rates became literally the highest? No one has been clearer in their arguments than Jonathan Haidt on this question. He argues that from 2010-2015, a “great re-wiring” shifted kids from a play-based childhood to a phone-based one. 2010 is when a lot of things quickly start getting worse for teens, especially. But if you carefully parse the data, it seems to affect girls more than boys. These changes were more punishing to teens than adults. Countries’ teen mental health gets worse only after social media use rises.
And why shouldn’t it? The Facebook Files show that they knew they were hacking the human brain. They intentionally used what is known of human psychology and neuroscience to make their products more addictive. Intermittent reinforcement, spaced learning, displaying group opinions and behaviors, the works. They experimented on children, running very scientifically valid randomized trials (“A / B Testing”) to see what was most addictive—absent the institutional review board, of course. The most brilliant minds of our generation spent their lives building machines that could extract human attention and sell it.
Our brightest— for two decades— declined careers attempting to cure cancer. It also wasn’t fashionable to work on clean energy. Instead, they chose the (more) lucrative salaries for building these attention vacuum machines. There was also money to be made financing those same companies—it’s been an almost singular focus of Venture Capital. The ever-rising valuations of their companies were validated by the consumption of more and ever more human attention and, thus, advertising dollars. This disruption of girlhood? It was fueled by endless money from venture investment, followed by mutual funds, 401k’s, and other pools of capital. These funds didn’t have to care why a return was happening. This state of affairs continued from 2010 to the present. Wealth was created. However, much like the Oil Boom, which befouled rivers to the point of combustion, there was toxic sludge, invisibly poisoning the childhood of girls.
The business model of social media companies like Facebook is to capture attention that could have been sold for at least minimum wage and, in many professionals’ cases, much more. Except—stay with me—they sell it for $1 per hour. That business model is why Meta Platforms is now valued at $1,730,000,000,000 as of the 7th of July, 2024. Taking human attention and selling it for less than it’s worth in any other context. Brilliant.
What was once the dastardly plan of Jim Carey’s Riddler in a campy Batman movie was achieved. Remember? We groaned as Edward Nygnma built “The Box” which could suck away human intelligence in Batman Forever? Don’t worry; the real-life Gavin Belsons built it back better as Instagram et. al. It worked. Silicon Valley was endlessly successful in capturing the world’s attention with its clever machines.
As it turns out, this was according to both second-tier Batman Plotline and biblical prophecy. In the book of Revelation, the author sees all manner of terrifying and awe-inspiring visions, from terrifying plagues and destruction to the unity of all humankind. We mean when we say something is “Apocolyptic?” This is because we are transliterating the Greek for “Revelation.” One of the prophecies is of the destruction of the city of Babylon, the symbol for all the evil in the world, particularly financial evil. The scene is as if you, the reader, have your back to the destruction of the city, looking at the evil merchants who escaped the destruction, only to watch in horror as their world burns. They lament that they will no longer be able to sell slaves. And, to the utter bafflement of the original first-century readers, they lament that they will no longer be able to sell psyches. Now, of course, we know there’s good business in that trade.
All was well in the world—E. Nygma raised round after round! Except people started dying. And not just anybody. Our daughters. And not just our daughters. Our young daughters. Some ancient people used to sacrifice young women to appease gods. “Carthage must be destroyed” was a rallying cry for Romans who would, even when all seemed hopeless, fight to the death to defeat the “advanced civilization” of Carthage. This city, home of Hannibal, stayed ahead by regularly sacrificing their children to Molech—a rather bloodthirsty god—on superheated metal idols. I’m sure the wealthy Carthaginian merchants had their reasons to feed their children to this god.
OM: Our metal idols? They only heat up when malfunctioning. However, it seems they sacrifice children just as well. This grief and loss keep us all in line, after all.
Thank you for reading The Frontier Psychiatrists. This post is public so feel free to share it.
Papini S, Hsin H, Kipnis P, et al. Validation of a multivariable model to predict suicide attempt in a mental health intake sample. JAMA Psychiatry. Published online March 27, 2024. doi:10.1001/jamapsychiatry.2024.0189
Solomon, T. M., Hajduk, M., Majernik, M., Jemison, J., Deschamps, A., Scoggins, J., ... & Barrow, R. (2023). Evaluating passive physiological data collection during Spravato treatment. Frontiers in Digital Health, 5, 1281529.
Dr. Owen Muir has a gift as an artist, journalist, clinician, psychiatrist, etc..... to see & describe a world that needs to be explored. We are in world 2024 where we need to “think” more & scroll less.
Tech is good or is it?
It is hard to believe that we are in same world where 2/3 of doctors once recommended cigarettes as a good / daily practice & now there is silence of big tech of the “harm” with social media except for chatter like less but still no impactful action, or consequences or the Surgeon General putting a warning label. The reality is they (BIG Tech /Social Media) know. They have the data. It is not being shared. Thank you Dr. Muir for your continued work! We need it. Our children need it!






Dr. Owen Muir has a gift as an artist, journalist, clinician, psychiatrist, etc..... to see & describe a world that needs to be explored. We are in world 2024 where we need to “think” more & scroll less.
Tech is good or is it?
It is hard to believe that we are in same world where 2/3 of doctors once recommended cigarettes as a good / daily practice & now there is silence of big tech of the “harm” with social media except for chatter like less but still no impactful action, or consequences or the Surgeon General putting a warning label. The reality is they (BIG Tech /Social Media) know. They have the data. It is not being shared. Thank you Dr. Muir for your continued work! We need it. Our children need it!
Every suicide is a tragedy. But the demographic with the highest suicide risk is older white men.